

- Department of Neurosurgery, Henry Ford Hospital, Detroit, Michigan, USA
- Department of Otolaryngology, Henry Ford Hospital, Detroit, Michigan, USA
Correspondence Address:
Jack Rock
Department of Neurosurgery, Henry Ford Hospital, Detroit, Michigan, USA
DOI:10.4103/sni.sni_412_17
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Lynn Mubita, Michael Seidman, Jack Rock. Internal auditory canal exostosis: A technical case report. 19-Mar-2018;9:64
How to cite this URL: Lynn Mubita, Michael Seidman, Jack Rock. Internal auditory canal exostosis: A technical case report. 19-Mar-2018;9:64. Available from: http://surgicalneurologyint.com/?post_type=surgicalint_articles&p=8814
Date of Submission
08-Nov-2017
Date of Acceptance
22-Jan-2018
Date of Web Publication
19-Mar-2018
Abstract
Background:Exostoses of the internal auditory canal is a rare finding that may present with disabling symptoms of dizziness, hearing loss, and vestibular dysfunction based on the extent of cranial nerve compression. The purpose of this case report is to discuss the presentation and outcomes in a patient who presented with this disorder.
Case Description:A 19-year-old female presented to the neurotologist with left ear discomfort, pain with left lateral gaze, and dizziness. She underwent extensive evaluation including audiometric testing, videonystagmography, and neuroimaging, which confirmed left auditory and vestibular hypofunction and compression of the contents of the internal auditory canal from the exostosis. After extensive counseling, the patient elected to undergo a suboccipital craniectomy to remove the internal auditory canal exostosis. She experienced complete resolution of symptoms.
Conclusions:Exostoses of the internal auditory canal, although rare, can present with severe symptoms of dizziness, hearing loss, and vestibular hypofunction based on the extent of cranial nerve compression. Imaging, particularly with thin-cut computed tomography, is invaluable in making the correct diagnosis. Severe cases can be treated successfully with surgery with minimal or no complications and excellent outcome.
Keywords: Exostoses, exostosis, hearing loss, internal auditory canal, osteoma, vertigo
BACKGROUND
Exostoses of the internal auditory canal are rare, and sometimes seen only on postmortem examinations. Not to be confused with osteomas of the external auditory canal, which are slow- growing tumors that arise from the tympano-squamous suture, exostoses of the internal auditory canal are broad-based elevations found anywhere in the tympanic bone.[
CLINICAL PRESENTATION
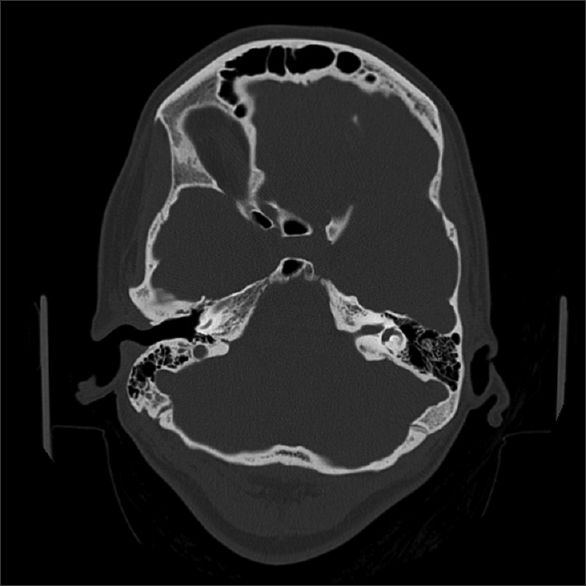
A 19-year-old female presented to a Neurotologic colleague with a several-month history of discomfort of the left ear that was exacerbated on left lateral gaze. In addition, she experienced dizziness triggered on sitting up and physical activity. Audiometric testing revealed minimal, bilateral low-frequency hearing loss, and videonystagmography demonstrated a 67% reduced vestibular response in the left ear. These symptoms were significantly impacting her quality of life. Past medical history was notable for thoracic outlet syndrome. She was otherwise intact on neurological examination. Thin-cut temporal bone computed tomography (CT) and magnetic resonance imaging (MRI) [Figures

Surgery was performed in lateral position, with the left side up [
Postoperatively, she was admitted to the neurosurgical intensive care unit where she was neurologically stable. Due to complaints of a low-pressure headache, she underwent blood patch with resolution of her headache. She was seen in follow-up 6 weeks later with neurosurgery and 7 weeks later in the neurotologic surgery clinic. She had mild discomfort around her left ear, but the episodes of dizziness as well as hearing difficulty had resolved. She remains symptom free and neurologically intact to this date.
DISCUSSION
Exostoses of the internal auditory canal are rare. The underlying cause of the exostoses is not understood.[
CONCLUSION
Exostoses of the internal auditory canal, although rare, can present with disabling and severe symptoms of dizziness, hearing loss, and vestibular dysfunction based on the extent of cranial nerve compression. Imaging, particularly with thin-cut CT, is invaluable in making the correct diagnosis. Severe cases can be successfully treated with surgery with minimal complications and excellent outcome.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Baik FM, Nguyen L, Doherty JK, Harris JP, Mafee MF, Nguyen QT. Comparative case series of exostoses and osteomas of the internal auditory canal. Ann Otol Rhinol Laryngol. 2011. 120: 255-60
2. Doan HT, Powell JS. Exostosis of the internal auditory canal. J Laryngol Otol. 1988. 102: 173-5
3. Nguyen LT, Baik FM, Doherty JK, Harris JP, Nguyen QT. Exostoses and osteomas of the internal auditory canal. Laryngoscope. 2010. p. S215-
4. Polat C, Baykara M, Ergen B. Evaluation of internal auditory canal structures in tinnitus of unknown origin. Clin Exp Otorhinolaryngol. 2014. 7: 160-4
5. Turetsky A, Vines F, Clayman A. Surfer's ear: Exostoses of the external auditory canal. Am J Neuroradiol. 1990. 11: 1217-8
6. Wright A, Corbridge R, Bradford R. Osteoma of the internal auditory canal. Br J Neurosurg. 1996. 10: 503-6

