

- Department of Neurology and Psychiatry, Neurosurgery, “Sapienza” University of Rome, Rome, Italy
- IRCCS Neuromed-Pozzilli, “Sapienza” University of Rome, Rome, Italy
- University Hospital Center Mother Theresa, Tirana, Albania
Correspondence Address:
Paolo Missori
IRCCS Neuromed-Pozzilli, “Sapienza” University of Rome, Rome, Italy
DOI:10.4103/2152-7806.193098
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Missori P, Domenicucci M, Paolini S, Mancarella C, Tola S, Alessandro D’Elia, Marotta N, Seferi A, Esposito V. Emergency decompressive craniectomy after removal of convexity meningiomas. Surg Neurol Int 26-Oct-2016;7:96
How to cite this URL: Missori P, Domenicucci M, Paolini S, Mancarella C, Tola S, Alessandro D’Elia, Marotta N, Seferi A, Esposito V. Emergency decompressive craniectomy after removal of convexity meningiomas. Surg Neurol Int 26-Oct-2016;7:96. Available from: http://surgicalneurologyint.com/surgicalint_articles/emergency-decompressive-craniectomy-removal-convexity-meningiomas/
Abstract
Background:Convexity meningiomas are benign brain tumors that are amenable to complete surgical resection and are associated with a low complication rate. The aim of this study was to identify factors that result in acute postoperative neurological worsening after the removal of convexity meningiomas.
Methods:Clinical evaluation and neuroradiological analysis of patients who underwent removal of a supratentorial convexity meningioma were reviewed. Patients were selected when their postoperative course was complicated by acute neurological deterioration requiring decompressive craniectomy.
Results:Six patients (mean age: 43.3 years) underwent surgical removal of a supratentorial convexity meningioma. Brain shift (mean: 9.9 mm) was evident on preoperative imaging due to lesions of varying size and perilesional edema. At various times postoperatively, patient consciousness worsened (up to decerebrate posture) with contralateral paresis and pupillary anisocoria. Computed tomography revealed no postoperative hematoma, however, did indicate increased brain edema and ventricular shift (mean: 12 mm). Emergency decompressive craniectomy and brief ventilator assistance were performed in all patients. Ischemia of the ipsilateral posterior cerebral artery occurred in 3 patients and hydrocephalus occurred in 2 patients. Outcome was good in 2, fair in 2, 1 patient had severe disability, and 1 patient died after 8 months.
Conclusions:Brain shift on preoperative imaging is a substantial risk factor for postoperative neurological worsening in young adult patients after the removal of convexity meningiomas. Emergency decompressive craniectomy must be considered because it is effective in most cases. Other than consciousness impairment, there is no reliable clinical landmark to guide the decision to perform decompressive craniectomy; however, brain ischemia may have already occurred.
Keywords: Brain, craniectomy, meningioma, shift, ventricular system
INTRODUCTION
Decompressive craniectomy is a function and life-saving procedure for patients with severe head injury, hemorrhagic or malignant ischemic stroke, and infectious diseases of the brain. These pathological events may lead to intracranial hypertension, brain swelling, and possible secondary diffuse ischemic damage that could cause brain death. Convexity meningiomas are a group of benign brain tumors that are amenable to complete surgical resection and are associated with a low complication rate.[
PATIENTS AND METHODS
Between January 2010 and April 2015, 123 consecutive patients underwent resection of a supratentorial convexity meningioma in our institutions. In six cases (4.8%), the postoperative course was complicated by acute or fast neurological decline that was unresponsive to maximized corticosteroid and osmotic therapies: Betamethasone 4 mg IV, mannitol 18% IV, 100 ml three times and six times daily, respectively. Patients in whom ischemia occurred as an intraoperative vessel injury were excluded from subsequent analysis. Preoperative and postoperative clinical courses as well as brain imaging were analyzed. Patients provided written informed consent to the surgical procedure and to the eventual publication of any accompanying image.
RESULTS
The 6 selected patients underwent surgical removal of a convexity meningioma (mean age: 43.3 years) [
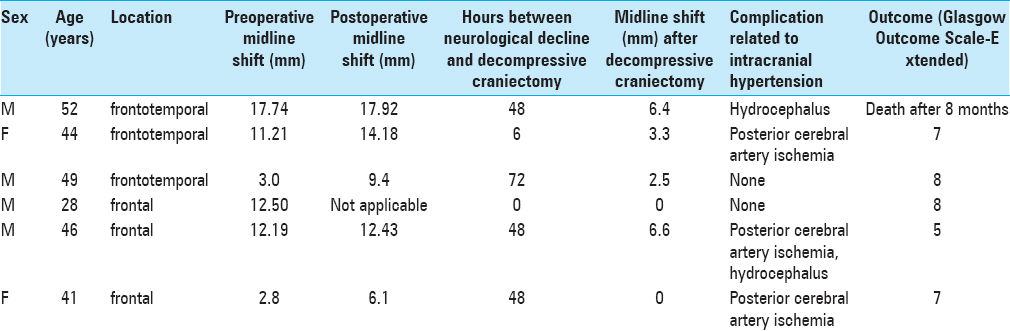
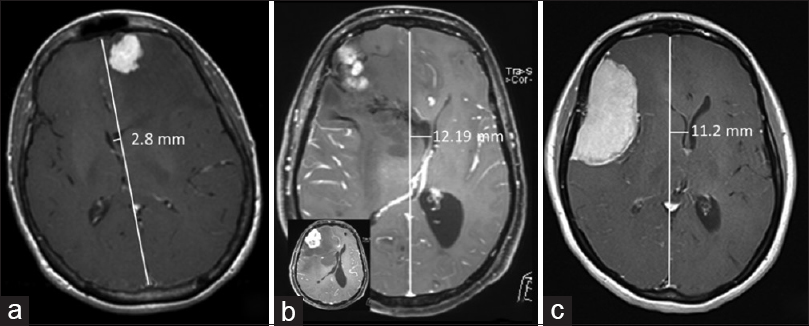
In the awakening phase, 1 patient displayed decerebrate posture and homolateral anisocoria, which prompted immediate reopening of the craniotomy site. Due to serious brain swelling, the edges of the craniotomy were enlarged and duraplasty was carried out. While the other 5 patients were under corticosteroid and osmotic therapies, fast progressive neurological impairment (worsening of consciousness and decerebrate posture in 1 patient, worsening of consciousness with contralateral motor impairment in 4 patients, and homolateral anisocoria in 3 patients) that was unresponsive to maximized medical therapies occurred 6–72 h after surgery (mean time to occurrence: 37 h). Computed tomography (CT) indicated that brain shift had increased by varying degrees in all 5 patients (mean shift: 12 mm) due to brain edema; no postoperative hematomas were evident, however, small intracavitary blood collection occurred in 2 patients, presumably as a secondary effect of the hindrance of venous outflow due to high intracranial pressure [
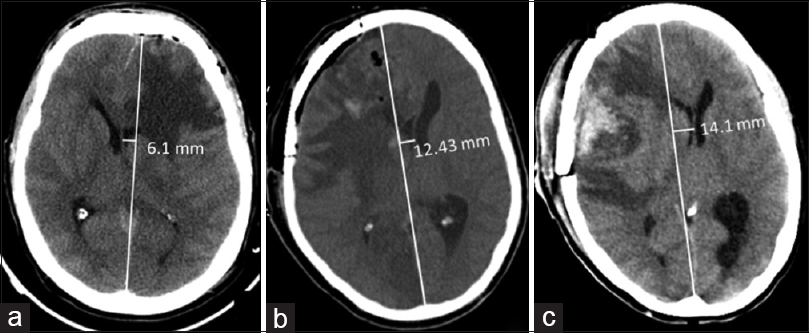
Figure 2
Emergent postoperative computed tomography revealed increased ventricular shift. Patients are shown left to right, as in
Cranioplasty was performed in all patients at 3–16 weeks (mean: 8 weeks) without complications. The 90-day mortality rate was 0%, however, 1 patient died after 8 months due to infectious disease and multiple organ failure. In other patients, at a mean follow-up of 14 months, the Glasgow Outcome Scores-Extended ranged from 5 to 8.
DISCUSSION
Serious neurological worsening can occur early after the surgical removal of a benign convexity meningioma. However, this complication has not received much attention in the literature. Here, clinical impairment in the early postoperative course was unexpected (in 1 patient it occurred immediately after surgical treatment), insidious, and very serious. It is plausible that surgical treatment and unwanted concomitant retraction injury presumably exacerbated pre-existing brain edema and ventricular shift, as demonstrated by control CT in the present investigation.
The preoperative mean midline shift in additional 111 preoperative images available in our retrospective study of convexity meningiomas was 6.2 mm and in the postoperative period was 7.3 mm. Although these results are not statistically significant, patients who experienced diminished consciousness had mean preoperative and postoperative midline shifts that were greater than that for patients who showed a normal postoperative clinical course.
Venous injury during surgical resection and postoperative hematoma were excluded. A surgeon should be aware that this fast neurological worsening is not related to the size of the meningioma because even a small convexity meningioma with marked edema can elicit this treacherous complication.
Clinical decline 24–48 h after uneventful meningioma resection is mentioned for lesions of the posterior cranial fossa.[
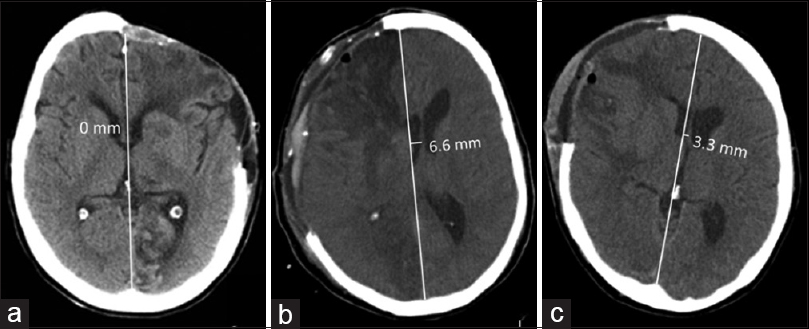
Here, our decision to remove the bone flap and to enlarge the bone edges for decompressive purposes appeared natural and mandatory in order to reverse the severe neurological worsening and marked ventricular shift on imaging, as is employed in patients suffering stroke or brain injury. An embarrassing dilemma is the lack of a firm indicator, other than the level of consciousness, that surgical decompression must be accomplished because an ischemic event in the posterior circulation may have already occurred. In all but 2 patients, decompressive craniectomy was implemented without modifying the skin incision; brain swelling prompted us to enlarge the bone margins as much as possible and to add a dural patch. This surgical choice immediately normalized the patients’ pupillary diameter and reduced ventricular shift on CT [
Ischemia in the territory of the posterior cerebral artery in 3 patients caused harsh intracranial hypertension and reduced cerebral blood flow, which we counteracted with decompressive craniectomy. The young adult age of our patients is notable.
In our clinical study of 6 patients, we observed a mean age 43.3 years. The remaining 117 patients harboring a convexity meningioma, and with an uncomplicated postoperative course, had a mean age of 57.3 years (range: 29–84 years). Due to the small sample size, this difference was not statistically significant.
The removal of convexity meningiomas with pre-existing edema yielded ventricular shift up to 10 mm in these young brains; young brains are less tolerant of intracranial mass effects than aged brains. Thus, the removal of convexity meningiomas must be considered highly risky in these patients.
In a previous series of 100 patients with a parasagittal meningioma invading the superior sagittal sinus, 3 patients (3%) died, presumably due to brain swelling.[
In conclusion, young adult patients with convexity meningiomas of various sizes associated with brain edema and ventricular shift up to 10 mm can deteriorate early after surgical removal of these lesions. When medical therapy fails, emergency decompressive craniectomy must be accomplished as early as possible to save the patient's neurological functions and life.
Patient consent
We have obtained fully informed, voluntary and written consent to publish from each patient whose case is described in the article.
All authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent- licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alvernia JE, Dang ND, Sindou MP. Convexity meningiomas: Study of recurrence factors with special emphasis on the cleavage plane in a series of 100 consecutive patients. J Neurosurg. 2011. 115: 491-8
2. Quiñones-Hinojosa A.editorsSchmidek and Sweet operative neurosurgical techniques: Indications, methods, and results. Philadelphia, PA: Elsevier/Saunders; 2012. p. 501-16
3. Asgari S, Bassiouni H, Hunold A, Klassen D, Stolke D, Sandalcioglu IE. Extensive brain swelling with neurological deterioration after intracranial meningioma surgery-Venous complication or ‘unspecific’ increase in tissue permeability. Zentralbl Neurochir. 2008. 69: 22-9
4. Elwatidy S. Bifrontal decompressive craniectomy is a life-saving procedure for patients with nontraumatic refractory brain edema. Br J Neurosurg. 2009. 23: 56-62
5. Hasseleid BF, Meling TR, Rønning P, Scheie D, Helseth E. Surgery for convexity meningioma: Simpson Grade I resection as the goal: Clinical article. J Neurosurg. 2012. 117: 999-1006
6. Lee JH.editors. Parasagittal meningiomas. Springer Science and Business Media, ed. Meningiomas: Diagnosis, Treatment, and Outcome. London: Springer-Verlag; 2009. p. 309-17
7. Nanda A, Vannemreddy P. Recurrence and outcome in skull base meningiomas: Do they differ from other intracranial meningiomas?. Skull Base. 2008. 18: 243-52
8. Ono K, Hatada J, Minamimura K, Ohara I, Wada K. Delayed enlargement of brain edema after resection of intracranial meningioma: Two case reports. Neurol Med Chir. 2009. 49: 478-81
9. Raza SM, Quiñones-Hinojosa A, Olivi A, DeMonte F, McDermott MW, Al-Mefty O.editors. Convexity Meningiomas. Al-Mefty's Meningiomas. New York: Thieme; 2011. p. 135-41
10. Sanai N, Sughrue ME, Shangari G, Chung K, Berger MS, McDermott MW. Risk profile associated with convexity meningioma resection in the modern neurosurgical era. J Neurosurg. 2010. 112: 913-9
11. Vignes JR, Sesay M, Rezajooi K, Gimbert E, Liguoro D. Peritumoral edema and prognosis in intracranial meningioma surgery. J Clin Neurosci. 2008. 15: 764-8
12. Yamaguchi S, Terasaka S, Kobayashi H, Asaoka K, Murata J, Houkin K. Giant skull base atypical meningioma presenting with rapidly progressive impaired consciousness caused by severe venous congestion: Case report. Neurol Med Chir. 2011. 51: 789-92
Commentary
- Editor-in-Chief E-mail:
jia@surgicalneurologyint.com
It has been my practice to leave the bone flap out in meningiomas, particularly if they are large and long standing, as they develop further swelling and can act as a mass. Just because it is a meningioma is not reason enough to replace the bone flap. One must think of the postoperative course, which inevitably produces edema. In large tumors, that can result in the complications you report. Usually, after leaving the flap out, the post-op course is more normal and the flap can be replaced later. You will find on repeat CTS that the edema is slow to resolve, so it may take up to two months to replace the bone flap.


