

- Department of Neurosurgery, Trauma and Burns Center, Ben Arous, Faculty of Medicine of Tunis, El Manar-Tunis University, Tunisia
Correspondence Address:
Ghassen Gader
Department of Neurosurgery, Trauma and Burns Center, Ben Arous, Faculty of Medicine of Tunis, El Manar-Tunis University, Tunisia
DOI:10.4103/sni.sni_411_17
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Mohamed Badri, Ghassen Gader, Kamel Bahri, Ihsen Zammel. Atypical imaging features of posterior fossa's dermoid cyst: Case report and review of literature. 07-May-2018;9:97
How to cite this URL: Mohamed Badri, Ghassen Gader, Kamel Bahri, Ihsen Zammel. Atypical imaging features of posterior fossa's dermoid cyst: Case report and review of literature. 07-May-2018;9:97. Available from: http://surgicalneurologyint.com/surgicalint-articles/atypical-imaging-features-of-posterior-fossas-dermoid-cyst-case-report-and-review-of-literature/
Date of Submission
07-Nov-2017
Date of Acceptance
29-Mar-2018
Date of Web Publication
07-May-2018
Abstract
Background:Intracranial dermoid cysts are uncommon lesions with characteristic imaging appearances. Symptomatic clinical presentation usually occurs in one of two ways: mass effect or rupture. Radiologically, dermoid cysts typically present as low density masses on computed tomography (CT) scan and are generally hyperintense on T1-weighted magnetic resonance imaging (MRI) sequences with variable signal on T2-weighted sequences.
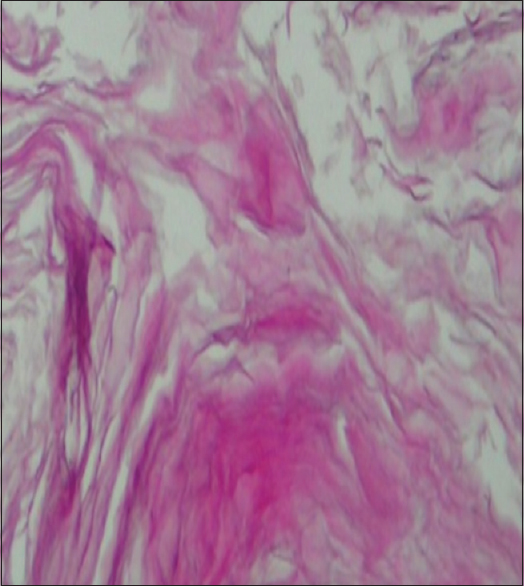
Case Description:We present the case of a 35-year-old female presented with symptoms of increased intracranial pressure. Radiological investigations showed a cystic posterior fossa tumor that was not only hyperdense on CT scans but also hypointense on MRI T1-weighted images. The patient underwent a total-gross resection of an extra-parenchymal posterior fossa tumor. Pathologic examination of the specimen concluded to dermoid cyst.
Conclusion:Dermoid cyst of the posterior fossa is a benign lesion surgically treatable. Only an appropriate radiological diagnosis of this lesion would permit a well-targeted therapeutic approach.
Keywords: Computed tomography, dermoid cyst, magnetic resonance imaging, posterior fossa
INTRODUCTION
Dermoid cysts are rare congenital lesions as a result of developmental malformation, with the defect in gastrulation affecting the surface ectoderm and causing a secondary disruption of neural tube closure.[
In this paper, we report a patient having fourth ventricle dermoid cyst with atypical radiololgical features.
CASE REPORT
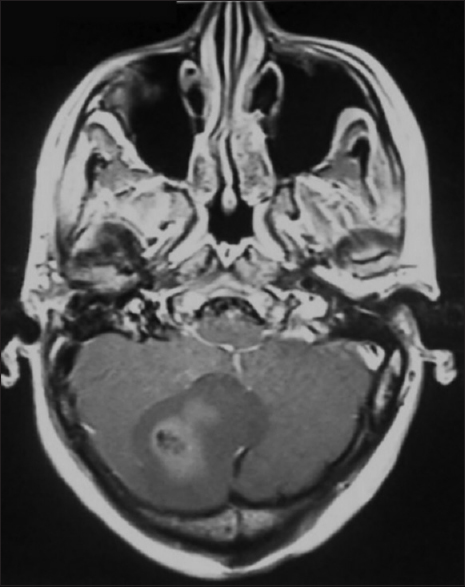
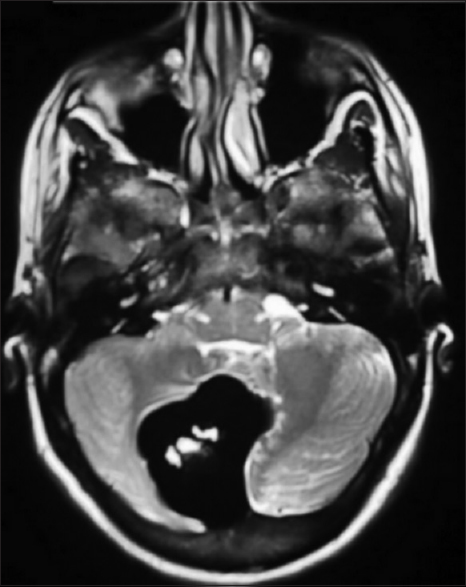
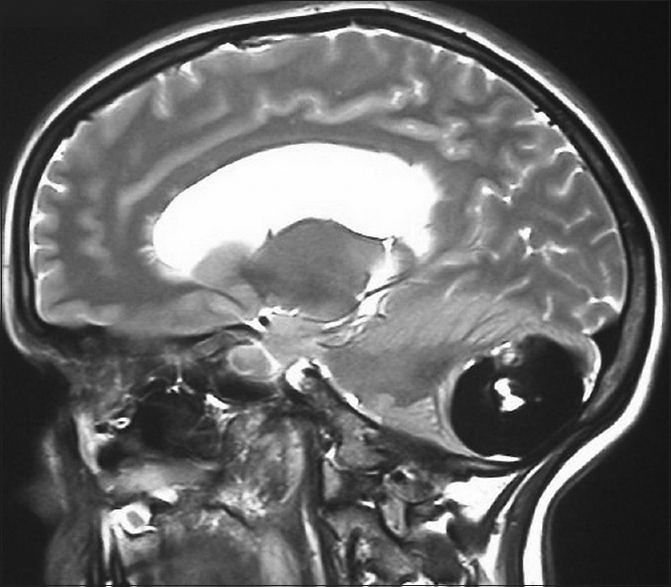
We report the case of a 35-year-old female presented with headaches, vomiting, and gradually worsening blurred vision. Physical examination was unremarkable except for a grade 2 papillary edema on the fundi. Brain CT scan showed imaging a large median and paramedian spontaneous homogenous hyperdense lesion in the posterior fossa. Mild surrounding edema and mass effect on the fourth ventricle was associated provoking a triventricular hydrocephalus [

DISCUSSION
The intracranial dermoid cyst is a rare entity, accounting for 0.1–0.7% of all intracranial tumors.[
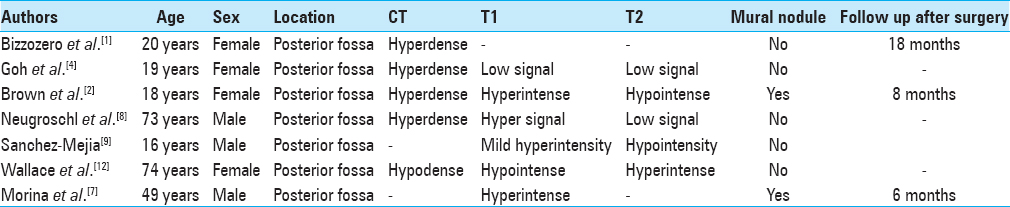
To our knowledge, nine cases have been reported about posterior fossa's dermoid cyst so far. All those cases are resumed in
The appearance of the dermoid cyst in typical cases is easily recognizable in imaging. They are usually extremely hypodense on CT scan with a Hounsfield unit (HU) of −20 to −140, explained by their lipid content.[
The unusual radiological finding in our patient was the hyperdensity on CT scan and the hyposignal on MRI T1-weighted images. The hyperdensity could be explained by the high protein content of the necrotic tissue within the lesion.[
CONCLUSION
The dermoid cyst of the posterior fossa is a benign lesion surgically treatable. The appropriate radiological diagnosis of this lesion permits a well-targeted therapeutic approach. The radiological study is often unequivocal during this lesion. Nevertheless, the hyperdense aspect of the lesion on CT associated with hyposignal on T1-weighted images on MRI may make the diagnosis of a dermoid cyst more difficult.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bizzozero L, Talamonti G, D'Angelo V, Casadei G, Arrigoni G, Collice M. Dermoid cyst mimicking hematoma in the posterior fossa. Clin Neurol Neurourg. 1992. 94: 61-3
2. Brown J, Morokoff A, Mitchell P. Unusual imaging appearance of an intracranial dermoid cyst. Am J Neuroradiol. 2001. 22: 1970-2
3. Douvoyiannis M, Goldman D, Abbott I, Litman N. Posterior fossa dermoid cyst with sinus tract and meningitis in a toddler. Pediatr Neurol. 2008. 39: 63-6
4. Goh G, Page R, Nixon T. An unusual CT and MR appearance of a posterior fossa dermoid cyst. Eur J Radiol. 1995. 20: 46-7
5. Lunardi P, Missori P, Gagliardi F, Fortuna A. Dermoid cysts of the posterior cranial fossa in children. Report of nine cases and review of the literature. Surg Neurol. 1990. 34: 39-42
6. Matthys M, Long S, Huisman T, Pindrik J, Tekes A. Posterior fossa dermoid cyst with a sinus tract and restricted diffusion on MR imaging: Value of structural imaging findings and signal characteristics. J Neuroradiol. 2012. 39: 134-5
7. Morina A, Kelmendil F, Morina Q, Morina D. Cerebellar dermoid cyst with contrast enhancement mural nodule. Acta Clin Croat. 2014. 53: 479-82
8. Neugroschl P, David N, Sadeghi A, Soebert B, Pirotte S, Rorive D. Unusual CT features of dermoid cyst in the posterior fossa. Eur Radiol. 2002. 12: 2726-9
9. Sanchez-Mejia R, Limbo M, Tihan T, Galvez M, Woodward M, Gupta N. Intracranial dermoid cyst mimicking hemorrhage. Case report and review of the literature. J Neurosurg. 2006. 105: 311-4
10. Sharma M, Sharma B, Yadav A, Khosla V. Posterior fossa dermoid in association with Klippel-Feil syndrome: A short report. Neurol India. 2001. 49: 210-2
11. Tan L, Kasliwal M, Harbhajanka A, Kellogg R, Arvanitis L, Munoz L. Hyperdense suprasellar mass: An unusual radiological presentation of intracranial dermoid cyst. J Clin Neurosci. 2015. 22: 1208-10
12. Wallace D, Tress B, Kwan P. Radiologically atypical congenital posterior fossa dermoid cyst presenting late in life. J Clin Neurosci. 2008. 15: 835-8
13. Wang Y, Chang T, Lo C, Tu M. Spontaneous rupture of intracranial dermoid cyst with chemical meningitis. J Emerg Med. 2013. 44: 275-6
14. Yasargil M, Abernathey C, Sarioglu A. Microneurosurgical treatment of intracranialdermoid and epidermoid cyst. Neurosurgery. 1989. 24: 561-7

