

Axial and oblique C2 pedicle diameters and feasibility of C2 pedicle screw placement: Technical note
- Department of Neurosurgery, University of Illinois at Chicago, Chicago, Illinois, USA
Correspondence Address:
Sergey Neckrysh
Department of Neurosurgery, University of Illinois at Chicago, Chicago, Illinois, USA
DOI:10.4103/sni.sni_438_17
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Dali Yin, Gerald Oh, Sergey Neckrysh. Axial and oblique C2 pedicle diameters and feasibility of C2 pedicle screw placement: Technical note. 16-Feb-2018;9:40
How to cite this URL: Dali Yin, Gerald Oh, Sergey Neckrysh. Axial and oblique C2 pedicle diameters and feasibility of C2 pedicle screw placement: Technical note. 16-Feb-2018;9:40. Available from: http://surgicalneurologyint.com/?post_type=surgicalint_articles&p=8779
Date of Submission
22-Nov-2017
Date of Acceptance
04-Jan-2018
Date of Web Publication
16-Feb-2018
Abstract
Background:For C2 pedicle screw placement/instrumentation, it is critical to adequately measure the axial and oblique C2 pedicle diameters utilizing the intraoperative O-arm.
Methods:Thirty-three patients who underwent C2 pedicle screw placement (2013–2016) utilizing the O-arm with tri-planar reconstruction. As O-arm software does not allow calibrated measurements with the application's measurement tool, we directly measured axial and oblique widths of the C2 pedicles on the screen with a regular ruler (e.g., “screen width of C2 pedicle”).
Results:The axial width of the C2 pedicles ranged from 6 to 15 mm on the right (mean 10.44 ± 2.15 mm) to 7 to 14 mm (10.29 ± 1.72 mm) on the left. The oblique width of C2 pedicles ranged from 10 to 19 mm on the right (mean, 14.73 ± 1.85 mm) and from 12 to 19 mm on the left (mean, of 15.33 ± 1.67 mm). These measurements indicated that oblique screen widths of the C2 pedicles were 1.4 and 1.5 times higher than their axial screen widths on the right and left sides, respectively.
Conclusions:The oblique screen widths of the C2 pedicles better predict the feasibility of C2 pedicle screw placement vs. their axial screen width as measured with a regular ruler.
Keywords: C2 pedicle width, O-arm, pedicle screw placement
INTRODUCTION
Three-dimensional intraoperative computed tomography (CT)-based O-arm surgical imaging facilitates C2 pedicle screw placement,[
PATIENTS AND METHODS
Patients
After institutional review board (IRB) approval, we retrospectively reviewed intraoperative O-arm placement of C2 pedicle screws in all 33 patients (2013–2016) [
Placement of C2 pedicle screws and posterior cervical fusion
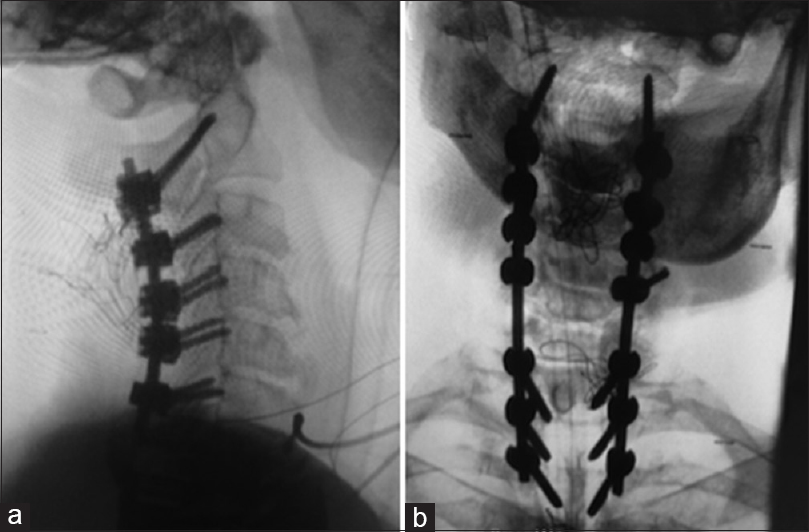
Prone and immobilized in a three-pin head holder, a linear incision was performed in the midline to expose the posterior elements of C2 and the cervical/thoracic vertebra, as needed. The C2 pedicle was palpated using a #1 Penfield instrument between the interspace of C1–C2; C2 pedicle screws were placed bilaterally using the free-hand technique. The O-arm spin was performed after C2 screws were placed to confirm their position [
O-arm surgical imaging system and measurements of C2 pedicle width
Utilizing the full spin technique combined with tri-planar reconstruction, the O-arm surgical imaging system (Medtronic, Inc. Minneapolis, MN) verifies intraoperative C2 screw placement. The widths of C2 pedicles were measured (mediolateral diameter of the pedicle isthmus, perpendicular to the pedicle axis) using a bone window for documentation of osseous anatomy. The right and left C2 pedicle diameters were measured on the axial images utilizing a regular ruler (e.g., in millimeters; “screen width of C2 pedicle”); this was followed by oblique pedicle measurements [
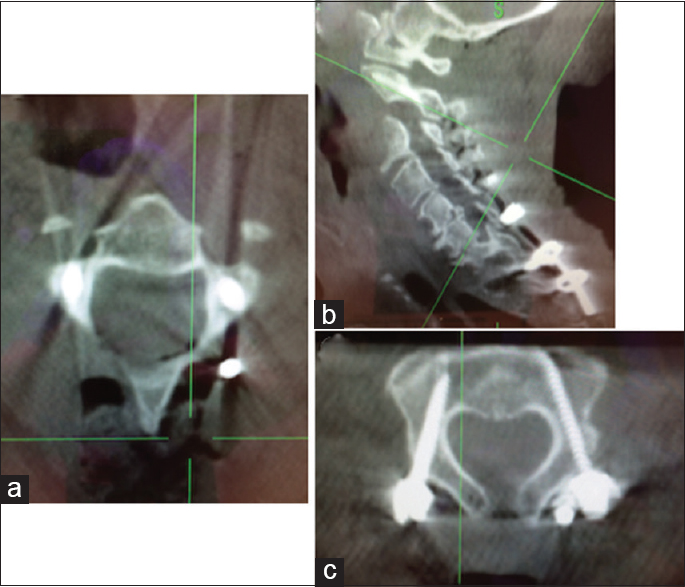
Figure 2
The axial (a) and oblique (c) widths of C2 pedicle on the screen were measured on the axial and oblique images using a regular ruler in millimeters, and therefore called “screen width of C2 pedicle”. The plane was positioned parallel to the C2 pedicle (b) using plane rotation function of the O-arm, oblique measurements (c) were then performed
Statistical analysis
Differences between axial and oblique width of C2 pedicles were analyzed with paired Student's t-test. Results are expressed as mean ± standard error (SEM). A P value of less than 0.05 was considered statistically significant.
RESULTS
The oblique screen widths of C2 pedicles were 1.4 and 1.5 times higher that axial screen widths on the right and left sides, respectively [

DISCUSSION
A major risk of C2 pedicle screw placement includes improper screw placement that may result in damaging the vertebral artery, the nerve roots, and/or spinal cord.[
The O-arm produced real-time three-dimensional images, providing information regarding C2 anatomy to more accurately place C2 screws. Of the 266 C2 screws placed in 133 patients addressing different cervical pathologies [
CONCLUSIONS
The intraoperative O-arm with multiplanar reconstruction facilitates C2 pedicle screw placement by allowing real-time on-screen measurement of the width (using a ruler) of the C2 pedicles.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chazono M, Soshi S, Inoue T, Kida Y, Ushiku C. Anatomical considerations for cervical pedicle screw insertion: The use of multiplanar computerized tomography reconstruction measurements. J Neurosurg Spine. 2006. 4: 472-7
2. Elliott RE, Tanweer O, Boah A, Smith ML, Frempong-Boadu A. Comparison of safety and stability of C2 pars and pedicle screws for atlantoaxial fusion: Meta-analysis and review of literature. J Neurosurg Spine. 2012. 17: 577-93
3. Jones EL, Heller JG, Silcox DH, Hutton WC. Cervical pedicle screws versus lateral mass screws. Anatomic feasibility and biomechanical comparison. Spine (Phila Pa 1976). 1997. 22: 977-82
4. Kotani Y, Cunningham BW, Abumi K, McAfee PC. Biomechanical analysis of cervical stabilization systems: An assessment of transpedicularscrew fixation in the cervical spine. Spine. 1994. 19: 2529-39
5. Le Pape S, Gauthe R, Latrove C, Cantogrel P, Proust F, Leroux J. Are C2 pedicles always screwable? Calibration and planning with a pedicle-lamina angle. Neurochirurgie. 2016. 62: 209-12
6. Schouten R, Lee R, Boyd M, Paquette S, Dvorak M, Kwon BK. Intra-operative cone-beam CT (O-arm) and stereotactic navigation in acute spinal trauma surgery. J Clin Neurosci. 2012. 19: 1137-43
7. Verma R, Krishan S, Haendlmayer K, Mohsen A. Functional outcome of computer-assisted spinal pedicle screw placement: A systematic review and meta-analysis of 23 studies including 5,992 pedicle screws. Eur Spine J. 2010. 19: 370-5
8. Vizurraga DE, Rhee JM, Borden TC, Mansour AS. “Inline” axial reconstructed CT scans provide a significantly larger assessment of C2 pedicle diameter for screw placement compared with “standard” axial scans: Implications for surgical planning. Clin Spine Surg. 2017. 30: E1039-45

