

- Department of Neuro-Surgery, Govind Ballav Pant Institute of Postgraduate Medical Education and Research (GIPMER), New Delhi, India
Correspondence Address:
Gautam Dutta
Department of Neuro-Surgery, Govind Ballav Pant Institute of Postgraduate Medical Education and Research (GIPMER), New Delhi, India
DOI:10.4103/sni.sni_47_18
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Gautam Dutta, Daljit Singh, Hukum Singh, Arvind K. Srivastava, Anita Jagetia, Atul Agrawal. Dorsal hemangioblastoma manifesting as holocord syringomyelia. 05-Apr-2018;9:73
How to cite this URL: Gautam Dutta, Daljit Singh, Hukum Singh, Arvind K. Srivastava, Anita Jagetia, Atul Agrawal. Dorsal hemangioblastoma manifesting as holocord syringomyelia. 05-Apr-2018;9:73. Available from: http://surgicalneurologyint.com/surgicalint-articles/dorsal-hemangioblastoma-manifesting-as-holocord-syringomyelia/
Date of Submission
08-Feb-2018
Date of Acceptance
21-Feb-2018
Date of Web Publication
05-Apr-2018
Abstract
Background:Intramedullary spinal hemangioblastomas are known to be accompanied by syringomyelia.
Case Description:Here, we report a patient who presented with symptoms of a Chiari malformation but was found to have a D4 intramedullary hemangioblastoma with a holocord syrinx.
Conclusions:Although rare, neurosurgeons should keep in mind the possibility of an intramedullary hemangioblastoma in patients presenting with symptoms of a Chiari malformation.
Keywords: Chiari malformation, differential diagnosis, hemangioblastoma, holocord, intramedullary, spinal, syringomyelia
INTRODUCTION
Spinal hemangioblastomas compromise 1.6–2.1% of all primary spinal cord tumors. They are located in cervical or thoracic region, and are typically highly vascular solid and/or cystic lesions. Although they may be associated with syringomyelia, they only rarely present with holocord syrinxes.[
CASE REPORT
A 21-year-old female presented with progressive numbness/tingling of the face, hands and feet, along with neck pain, gait instability, and hesitancy/urge incontinence of 6 months duration. On examination she exhibited weakness of both the upper and lower extremities along with the inability to feel hot/cold, and loss of pain sensation in both upper limbs and trunk. On examination, she exhibited a spastic quadriparesis (power 4/5) with atrophy in all four limbs. Reflexes were brisk bilaterally in all four extremities and she had bilateral Babinski responses. Dissociative sensory loss was present from T1 to T12 dermatomes bilaterally. Urodynamic study revealed detrusor hyperreflexia with sphincter dysynergia, requiring an indwelling Foley's catheter.
Diagnostic studies
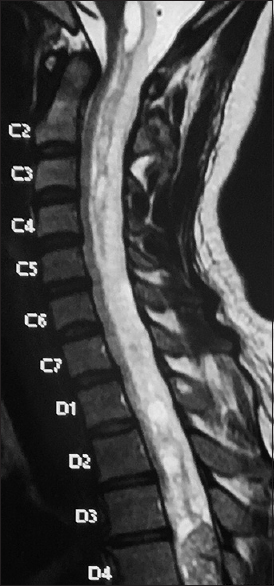
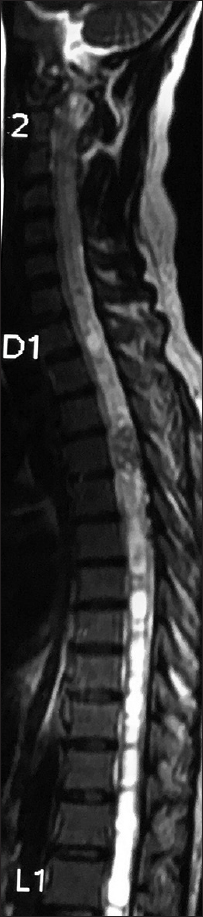
The cervicothoracic magnetic resonance imaging (MRI) revealed a well-defined 14 × 15 × 25 mm lesion at the D4 level. It was isointense on T1, heterogeneously hyperintense T2, and intensely enhanced within the cord at the D4 level. Additionally, it showed cystic degeneration with collateral channels on the surface [
Surgery
The patient underwent a near total surgical excision of the lesion. The histology confirmed a WHO grade 1 hemangioblastoma. Thorough ophthalmological, abdominal, and brain evaluation documented no additional lesions that could be attributed to von Hippel–Lindau (VHL) syndrome.
Postoperative course
The patient ambulated by the end of the first postoperative week; she can now walk without support. Although urodynamic studies showed significant improvement, she still requires intermittent catheterization.
DISCUSSION
Syringomyelia is seen mainly in association with Chiari malformation, inflammatory pathologies, infarction, trauma, and intramedullary spinal cord tumors. Syrinxes with the latter are variously attributed to transudation of fluid from the tumor vessels, obstruction to cerebrospinal fluid (CSF), and/or obstruction of extracellular fluid flow. The subarachnoid and the extracellular spaces are a single fluid compartment with interrelated fluid flow; a block in one of the spaces may be reflected as increased flow in the other. Of interest, the higher the level of the tumor the greater the incidence of the accompanying syrinx.[
In this case, holocord syrinx formation occurred both rostral and caudal to the D4 hemangioblastoma. Here, we postulate the syrinx could be attributed both to obstruction of CSF flow and transudation of highly proteinous tumor fluid.
Although holocord syringomyelia has also been most frequently reported in conjunction with Chiari malformations,[
CONCLUSION
Although most patients presenting with holocord syrnigomyelia, are thought to have Chiari malformations, others may have focal intramedullary spinal cord tumors. Therefore, it is critical to assess the entire spine to avoid missing these lesions and the opportunity to correctly treat these patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Kumar J, Kumar A, Gupta S. Chiari I malformation with holocord syrinx. J Neurol Neurosurg Psychiatry. 2007. 78: 146-
2. Pai SB, Krishna KN. Secondary holocord syringomyelia with spinal hemangioblastoma: A report of two cases. Neurol India. 2003. 51: 67-8
3. Wu TC, Guo WY, Lirng JF, Wong TT, Chang FC, Luo CB. Spinal cord hemangioblastoma with extensive syringomyelia. J Chin Med Assoc. 2005. 68: 40-4


JESUS FARINAS YANES
Posted January 30, 2020, 11:24 am
Congratulations for your very interesting case report and the excellent evolution of the patient.