

- Department of Neurosurgery, Westchester Medical Center, New York Medical College, Valhalla, New York, USA
- Department of Neurology, Westchester Medical Center, New York Medical College, Valhalla, New York, USA
- Capital Institute for Neurosciences, Stroke and Cerebrovascular Center, Capital Health System, Trenton, New Jersey, USA
Correspondence Address:
Arthur Wang
Capital Institute for Neurosciences, Stroke and Cerebrovascular Center, Capital Health System, Trenton, New Jersey, USA
DOI:10.4103/2152-7806.210993
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Arthur Wang, Noorie Pednekar, Rachel Lehrer, Akira Todo, Ramandeep Sahni, Stephen Marks, Michael F. Stiefel. DRAGON score predicts functional outcomes in acute ischemic stroke patients receiving both intravenous tissue plasminogen activator and endovascular therapy. 18-Jul-2017;8:149
How to cite this URL: Arthur Wang, Noorie Pednekar, Rachel Lehrer, Akira Todo, Ramandeep Sahni, Stephen Marks, Michael F. Stiefel. DRAGON score predicts functional outcomes in acute ischemic stroke patients receiving both intravenous tissue plasminogen activator and endovascular therapy. 18-Jul-2017;8:149. Available from: http://surgicalneurologyint.com/surgicalint-articles/dragon-score-predicts-functional-outcomes-in-acute-ischemic-stroke-patients-receiving-both-intravenous-tissue-plasminogen-activator-and-endovascular-therapy/
Date of Submission
05-Nov-2016
Date of Acceptance
18-Dec-2016
Date of Web Publication
18-Jul-2017
Abstract
Background:The DRAGON score, which includes clinical and computed tomographic (CT) scan parameters, predicts functional outcomes in ischemic stroke patients treated with intravenous tissue plasminogen activator (IV tPA). We assessed the utility of the DRAGON score in predicting functional outcome in stroke patients receiving both IV tPA and endovascular therapy.
Methods:A retrospective chart review of patients treated at our institution from February 2009 to October 2015 was conducted. All patients with computed tomography angiography (CTA) proven large vessel occlusions (LVO) who underwent intravenous thrombolysis and endovascular therapy were included. Baseline DRAGON scores and modified Rankin Score (mRS) at the time of hospital discharge was calculated. Good outcome was defined as mRS ≤3.
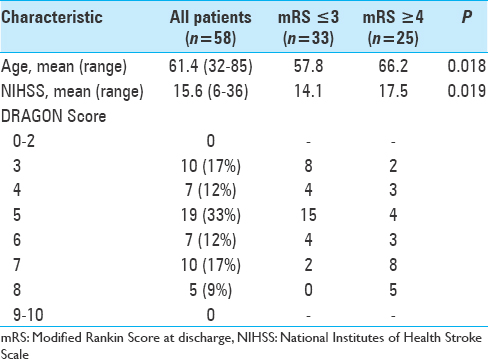
Results:Fifty-eight patients with LVO of the anterior circulation were studied. The mean DRAGON score of patients on admission was 5.3 (range, 3–8). All patients received IV tPA and endovascular therapy. Multivariate analysis demonstrated that DRAGON scores ≥7 was associated with higher mRS (P P
Conclusions:The DRAGON score can help predict better functional outcomes in ischemic stroke patients receiving both IV tPA and endovascular therapy. This data supports the use of the DRAGON score in selecting patients who could potentially benefit from more invasive therapies such as endovascular treatment. Larger prospective studies are warranted to further validate these results.
Keywords: Endovascular thrombectomy, ischemic stroke, large vessel occlusion, tissue plasminogen activator
INTRODUCTION
Intravenous tissue plasminogen activator (IV tPA) has been shown to improve functional outcomes in patients with acute ischemic strokes secondary to large vessel occlusions (LVO).[
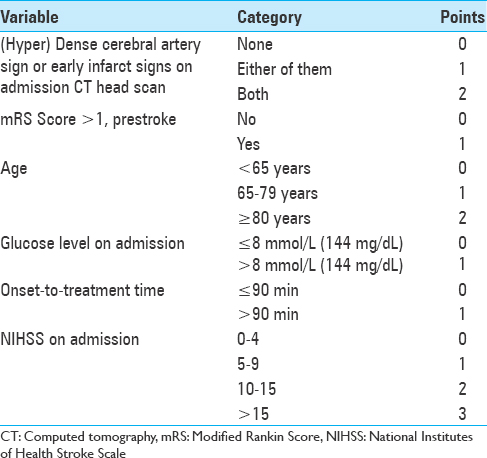
The DRAGON score is a 10-point scoring system based on computed tomography (CT) findings of hypoDensity or a dense MCA sign, prestroke modified Rankin Scale (mRS), Age, Glucose level on admission, Onset-to-treatment time, and initial National Institutes of Health Stroke Score (NIHSS).[
Recent randomized clinical trials using modern endovascular techniques have demonstrated the efficacy of endovascular stroke therapy for treating patients with acute ischemic strokes from LVO.[
MATERIALS AND METHODS
Institutional Review Board approval was obtained prior to study initiation. A retrospective chart review was conducted among anterior circulation ischemic stroke patients treated with IV tPA and endovascular therapy, with either the ADAPT technique or stent-triever. The major inclusion criteria were anterior circulation LVO seen on computed tomography angiography (CTA) and age ≥18. Anterior circulation LVO was defined as occlusions of the internal carotid artery (ICA) and M1 and/or M2 segment of the middle cerebral artery (MCA). Baseline DRAGON scores [
All endovascular interventions were performed on a flat detector-based biplane angiographic system under general anesthesia. Endovascular treatment included mechanical thrombectomy with or without intraarterial thrombolysis (intraarterial tissue plasminogen activator). Mechanical thrombectomy was defined as a stentriever and/or direct aspiration via a large-bore (≥5 Fr) intracranial reperfusion catheter. The degree of recanalization (Thrombolysis in Cerebral Infarction, TICI score) was determined at the end of the case by an endovascular surgeon.
The primary clinical outcome was the modified Rankin Scale (mRS) score at discharge. All mRS scores were reported on physical therapy progress notes and reviewed by stroke neurologists. Good outcome was defined as a mRS score 0–3 and poor outcome as mRS 4–6 (death or dependency).
Univariate analysis for predictors of outcome were determined using the χ2 and Student's t-test. Means were compared using the Student's t-test (two-tailed), and percentages were compared using the χ2 test. P values ≤0.05 were considered significant. Statistical analysis was performed using NCSS Statistical Software Inc V10.0 (Salt Lake City, Utah).
RESULTS
During the study period, a total of 58 patients met the inclusion criteria [
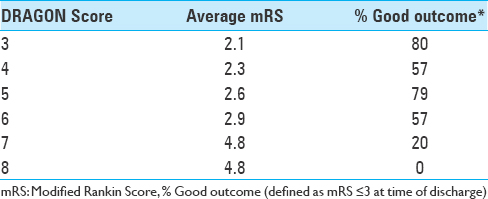
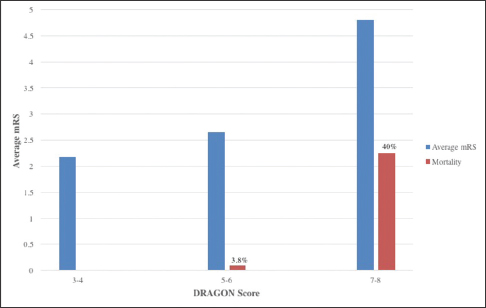
The highest and lowest percentage of good outcomes (mRS ≤ 3) was found in patients with a DRAGON score of 3 and 8, respectively. With increasing DRAGON scores, worse clinical outcome (mRS ≥ 4) was observed [
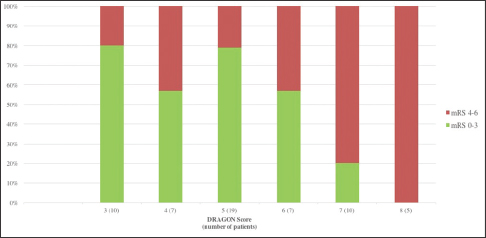
The association between subgroups of DRAGON scores and mRS and mortality rate is shown in
DISCUSSION
The DRAGON score was originally proposed as an easy way of identifying patients who should be given additional therapeutic interventions (i.e., endovascular, hypothermia) due to poor functional outcomes after IV tPA.[
Although the DRAGON score has been validated by several centers across the world, there are no studies investigating the utility of the score in predicting functional outcomes of patients receiving both IV tPA and endovascular therapy.[
There exist a few scoring systems in the literature that have shown promise in predicting the clinical outcome, and thus, appropriately select patients for endovascular therapy. The CTA collateral score, based on the degree of collateral circulation on pretreatment CTA, has been shown to predict smaller infarct volumes and better clinical outcomes in patients after recanalization with endovascular intervention.[
Compared with other scoring systems, the DRAGON score is (1) fast to obtain, (2) consists of parameters known at admission, and (3) has a low cost; free.[
A few limitations need to be acknowledged in our current study. First, despite controlling for established stroke outcome predictors, we cannot rule out additional baseline confounding variables that can affect patient outcomes. Second, this study uses data from only one center. Our aim was to apply an already established scoring system towards predicting stroke outcomes rather than investigate a novel prognostic tool. Third, as we only included anterior circulation strokes, our study results cannot be applied to posterior circulation strokes. Further data is needed to determine if the DRAGON score can be adapted for posterior circulation strokes.
CONCLUSIONS
The DRAGON score is a fast and easy score to obtain that can predict the functional outcomes of acute ischemic stroke patients treated with IV tPA and endovascular therapy. Larger prospective studies and external validation of the score as it applies to both IV tPA and endovascular therapy is warranted.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Adeoye O, Hornung R, Khatri P, Kleindorfer D. Recombinant tissue-type plasminogen activator use for ischemic stroke in the United States: A doubling of treatment rates over the course of 5 years. Stroke. 2011. 42: 1952-5
2. Baek JH, Kim K, Lee YB, Park KH, Park HM, Shin DJ. Predicting Stroke Outcome Using Clinical versus Imaging-based Scoring System. J Stroke Cerebrovasc Dis. 2015. 24: 642-8
3. Bhatia R, Hill MD, Shobha N, Menon B, Bal S, Kochar P. Low rates of acute recanalization with intravenous recombinant tissue plasminogen activator in ischemic stroke. Stroke. 2010. 41: 2254-8
4. Cooray C, Mazya M, Bottai M, Dorado L, Skoda O, Toni D. External Validation of the ASTRAL and DRAGON Scores for Prediction of Functional Outcome in Stroke. Stroke. 2016. 47: 1493-9
5. Elijovich L, Goyal N, Mainali S, Hoit D, Arthur AS, Whitehead M. CTA collateral score predicts infarct volume and clinical outcome after endovascular therapy for acute ischemic stroke: A retrospective chart review. J Neurointervent Surg. 2016. 8: 559-62
6. Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008. 359: 1317-29
7. IST-3 collaborative group, Sandercock P, Wardlaw JM, Lindley RI, Dennis M, Cohen G. The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): A randomised controlled trial. Lancet. 2012. 379: 2352-63
8. Labeyrie PE, Redjem H, Blanc R, Labeyrie MA, Bartolini B, Ciccio G. The Capillary Index Score before thrombectomy: An angiographic correlate of favorable outcome. J Neurointervent Surg 2015. 2015. p. 1-4
9. Ovesen C, Christensen A, Nielsen JK, Christensen H. External validation of the ability of the DRAGON score to predict outcome after thrombolysis treatment. J Clin Neurosci. 2013. 20: 1635-6
10. Rangaraju S, Aghaebrahim A, Streib C, Sun CH, Ribo M, Muchada M. Pittsburgh Response to Endovascular therapy (PRE) score: Optimizing patient selection for endovascular therapy for large vessel occlusion strokes. J Neurointervent Surg. 2015. 7: 783-8
11. Saqqur M, Uchino K, Demchuk AM, Molina CA, Garami Z, Calleja S. Site of arterial occlusion identified by transcranial Doppler predicts the response to intravenous thrombolysis for stroke. Stroke. 2007. 38: 948-54
12. Strbian D, Meretoja A, Ahlhelm FJ, Pitkäniemi J, Lyrer P, Kaste M. Predicting outcome of IV thrombolysis-treated ischemic stroke patients: The DRAGON Score. Neurology. 2012. 78: 427-32
13. Strbian D, Seiffge DJ, Breuer L, Numminen H, Michel P, Meretoja A. Validation of the DRAGON Score in 12 Stroke Centers in Anterior and Posterior Circulation. Stroke. 2013. 44: 2718-21

