

- Aga Khan University Medical College, Karachi, Pakistan
- Department of Medicine, Aga Khan University, Karachi, Pakistan
Correspondence Address:
Amir H. Sohail
Department of Medicine, Aga Khan University, Karachi, Pakistan
DOI:10.4103/sni.sni_364_17
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Amir H. Sohail, Muhammad A. A. Maan, Muhammad S. Khan, Qamar Masood. Isolated ligamentum flavum ossification in primary hypoparathyroidism. 10-Jan-2018;9:4
How to cite this URL: Amir H. Sohail, Muhammad A. A. Maan, Muhammad S. Khan, Qamar Masood. Isolated ligamentum flavum ossification in primary hypoparathyroidism. 10-Jan-2018;9:4. Available from: http://surgicalneurologyint.com/surgicalint-articles/isolated-ligamentum-flavum-ossification-in-primary-hypoparathyroidism/
Date of Submission
27-Sep-2017
Date of Acceptance
26-Oct-2017
Date of Web Publication
10-Jan-2018
Abstract
Background:The ligamenta flava can undergo ossification and calcification resulting in myelopathy. Only seven cases of ligamentum flavum ossification in association with hypoparathyroidism have been reported, most of which had concurrent osseous changes in other spinal ligaments. Here, we report a patient with hypoparathyroidism who presented with ligamentum flavum ossification causing both cervical and thoracic myelopathy.
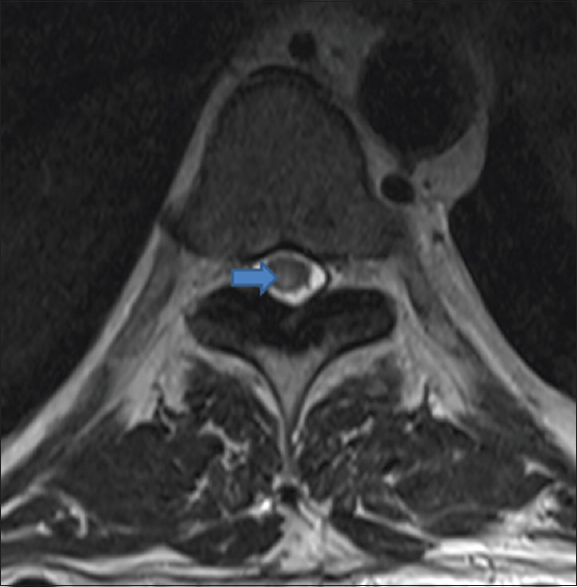
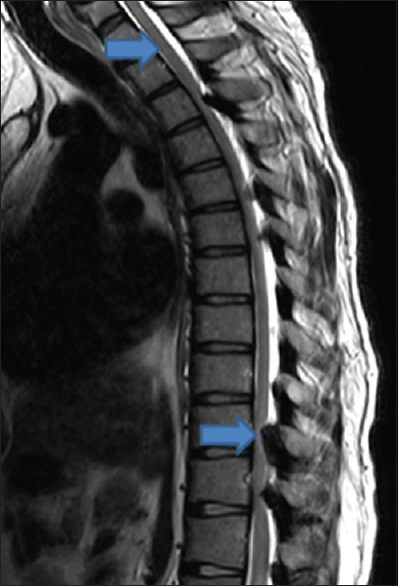
Case Description:A 43-year-old male presented with backache, urinary retention, and lower limb weakness for the last few days. Magnetic resonance imaging scan showed ossification of the ligamentum flavum in the cervical and thoracic regions, with severe spinal stenosis. Following spinal decompressive surgery, the patient made a complete recovery. Primary hypoparathyroidism was found to be the underlying cause for ligamentum flavum ossification.
Conclusion:Ossification of ligamentum flavum secondary to hypoparathyroidism should be considered as a possible cause of myelopathy in all patients presenting with symptoms of spinal cord compression.
Keywords: Hypoparathyroidism, ligamentum flavum, myelopathy, ossification, parathyroid hormone
INTRODUCTION
Degenerative calcification/ossification of the ligamentum flavum (OLF) often affects the geriatric Asian population. Although it is most prominent in the Japanese, it is only rarely found in the Pakistani population.[
OLF, resulting in thoracic myelopathy, is most frequently attributed to hypoparathyroidism, as well as to other factors and conditions (e.g. vitamin D, parathyroid hormone (PTH), local tissue growth factors, insulin, hyperthyroidism, hemochromatosis) [
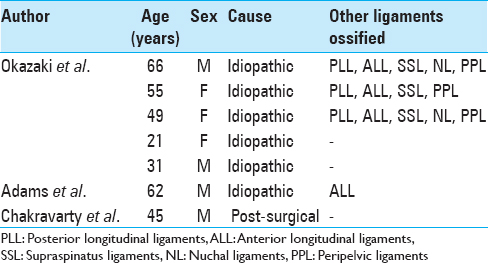
Table 1
Causes for ligamentum flavum ossification reported in literature[
CASE PRESENTATION
A 43-year-old Punjabi male presented with backache, lower extremity weakness, and urinary retention of several days duration. He had fallen from a height of three feet while working in the fields the previous week. The neurological examination was consistent with a severe spastic paraplegia; marked lower extremity weakness/paraparesis (1/5), bilateral diffuse hyperreflexia, and bilateral Babinski responses.
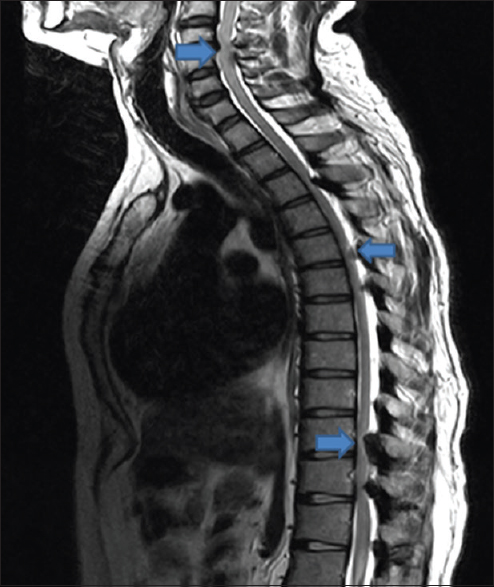
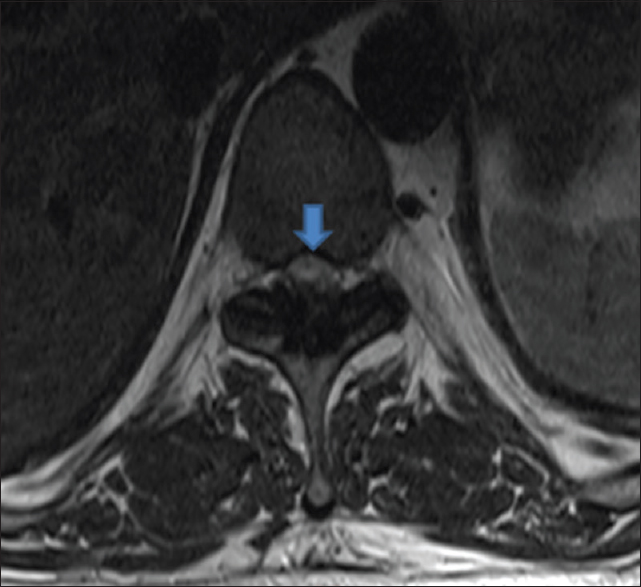
Magnetic resonance imaging (MRI) scan of the spine showed multilevel OLF with marked spinal cord compression at the C4-C5 and T10-T11 levels [Figures
The patient underwent laminectomies at the C4-C5, T3-T4, and T10-T11 levels. Intraoperatively, the patient sustained an acute myocardial infarction. Calcium and phosphorus studies were consistent with the diagnosis of primary hypoparathyroidism; low ionized calcium level (1.99 mg/dL), low calcium level (4.2 mg/dL), low corrected calcium (5.0 mg/dL), low magnesium (0.9 mg/dL), high phosphorus (7.7 mg/dL), and a low parathyroid hormone level (<3.0 pg/ml). The patient was treated with intravenous calcium gluconate and magnesium, and oral calcium, magnesium, and vitamin D.
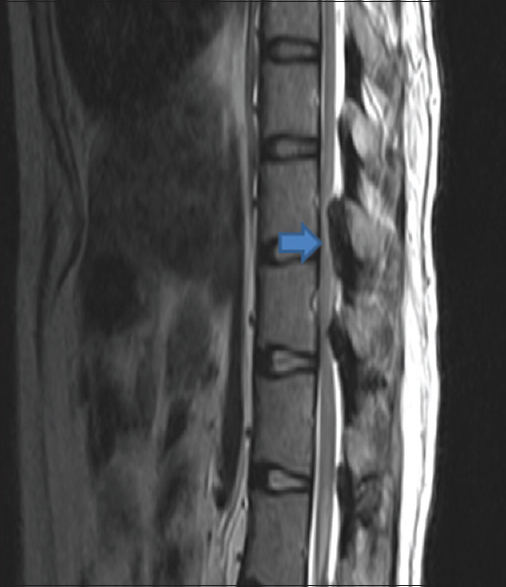
The postoperative MRI scans documented adequate OLF removal at the C4-C5 and T10-T11 levels [

DISCUSSION
Patients with OLF can present with myelopathy due to cervical and/or thoracic cord compression [
The pathophysiology of OLF, most typically attributed to hypoparathyroidism, is incompletely understood.[
About 50% of patients with thoracic myelopathy due to OLF will improve.[
CONCLUSION
Ossification of ligamentum flavum is a possible cause of myelopathy in patients with symptoms of spinal cord compression. If OLF is present, laboratory investigations should include a workup for hypoparathyroidism. Most critically, when myelopathy is significant, prompt surgical decompression is warranted.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initial will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Adams JE, Davies M. Paravertebral and peripheral ligamentous ossification: An unusual association of hypoparathyroidism. Postgrad Med J. 1977. 53: 167-72
2. Ahn DK, Lee S, Moon SH, Boo KH, Chang BK, Lee J. Ossification of the Ligamentum Flavum. Asian Spine J. 2014. 8: 89-96
3. Aizawa T, Sato T, Sasaki H, Matsumoto F, Morozumi N, Kusakabe T. Results of surgical treatment for thoracic myelopathy: Minimum 2-year follow-up study in 132 patients. J Neurosurg Spine. 2007. 7: 13-20
4. Chakravarty A, Anand S, Sapra H, Mehta Y. Undetected hypoparathyroidism: An unusual cause of perioperative morbidity. Indian J Anaesth. 2014. 58: 470-
5. Hur H, Lee J, Lee J, Kim J, Kim S. Thoracic Myelopathy Caused by Ossification of the Ligamentum Flavum. J Korean Neurosurg Soc. 2009. 46: 189-
6. Kang K, Lee C, Shin S, Park S, Chung C, Chung S. Ossification of the ligamentum flavum of the thoracic spine in the Korean population. J Neurosurg Spine. 2011. 14: 513-9
7. Li H, Jiang L, Dai L. Hormones and growth factors in the pathogenesis of spinal ligament ossification. Eur Spine J. 2007. 16: 1075-84
8. Okazaki T, Takuwa Y, Yamamoto M, Matsumoto T, Igarashi T, Kurokawa T. Ossification of the paravertebral ligaments: A frequent complication of hypoparathyroidism. Metabolism. 1984. 33: 710-3
9. Park B, Min W, Oh C, Jeon I, Kim S, Kyung H. Surgical outcome of thoracic myelopathy secondary to ossification of ligamentum flavum. Joint Bone Spine. 2007. 74: 600-5
10. Seichi A, Hoshino Y, Kimura A, Nakahara S, Watanabe M, Kato T. Neurological Complications of Cervical Laminoplasty for Patients With Ossification of the Posterior Longitudinal Ligament—A multi-Institutional Retrospective Study. Spine. 2011. 36: E998-E1003
11. Shen HX, Li L, Yang ZG, Hou TS. Position of increased signal intensity in the spinal cord on MR images: Does it predict the outcome of cervical spondylotic myelopathy.?. Chin Med J (Engl). 2009. 122: 1418-22
12. Shiraishi T, Crock HV, Lewis P. Thoracic myelopathy due to isolated ossification of the ligamentum flavum. J Bone Joint Surg. 1995. 77-B: 131-3

