

- Department of Neurosurgery, Sylvanus Olympio University Hospital Center, Togo
- Department of Radiology, Sylvanus Olympio University Hospital Center, Togo
- Department of Intensive Care Unit, Sylvanus Olympio University Hospital Center, Togo
Correspondence Address:
E. Kpelao
Department of Intensive Care Unit, Sylvanus Olympio University Hospital Center, Togo
DOI:10.4103/sni.sni_159_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: E. Kpelao, K. A. Beketi, K. M. H. Ahanogbe, A. K. Moumouni, A. K. Doleagbenou, K. Egu, B. Ntimon, M. Tchaou, P. Egbohou. Middle meningeal artery aneurysm: Case report. 01-Aug-2017;8:172
How to cite this URL: E. Kpelao, K. A. Beketi, K. M. H. Ahanogbe, A. K. Moumouni, A. K. Doleagbenou, K. Egu, B. Ntimon, M. Tchaou, P. Egbohou. Middle meningeal artery aneurysm: Case report. 01-Aug-2017;8:172. Available from: http://surgicalneurologyint.com/surgicalint-articles/middle-meningeal-artery-aneurysm-case-report/
Date of Submission
24-Apr-2017
Date of Acceptance
16-Jul-2017
Date of Web Publication
01-Aug-2017
Abstract
Background:Aneurysms of meningeal middle artery (MMA) are extremely rare. These aneurysms are of two types: true aneurysm and pseudoaneurysm. The true type is usually seen with pathologic conditions. Pseudoaneurysms, on the other hand, are associated with a skull fracture. Epilepsy caused by MMA aneurysm has never been described to our knowledge. We report a case of true aneurysm isolated from MMA revealed by epilepsy.
Case Description:A 57-year-old patient with a history of high blood pressure developed epilepsy which was treated by valproic acid. Initial scalp electroencephalography (EEG) showed seizure activity arising from the right temporal area. Epilepsy had become drug-resistant. Cerebral angiography revealed an aneurysm of the right middle meningeal artery without any other intraparenchymal anomaly. The interrogation did not reveal any history of family aneurysm. The patient underwent surgery with coagulation of the aneurysm and the MMA. The aneurysm was intradural in contact with the temporal cortex, and the surrounding brain tissues were preserved. The operative follow-up was favorable with amelioration of convulsions with a single antiepileptic. We planned to stop antiepileptic treatment according to electroencephalograms.
Conclusions:Aneurysms of the MMA are rare. Their mode of revelation by seizures is unusual. The factors of rupture are not known. When isolated, their physiopathology is identical to that of the aneurysms of the Willis polygon. Their management uses the same techniques as for other cerebral aneurysms.
Keywords: Aneurysm, epilepsy, middle meningeal artery
INTRODUCTION
Aneurysms of the meningeal middle artery (MMA) are extremely rare in comparison with the frequency of cerebral aneurysms. Aneurysms of the MMA are of two types: true aneurysm and pseudoaneurysm.[
CASE REPORT
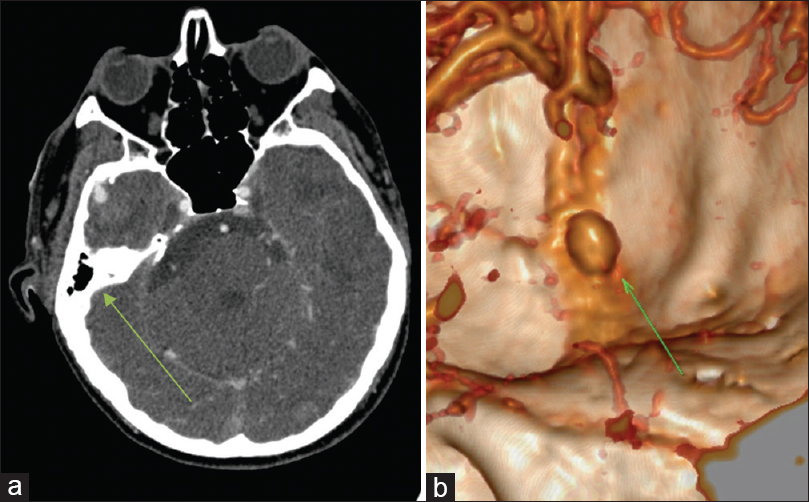
A 57-year-old patient, nonsmoker and occasional drinker, with a history of high blood pressure who had suffered from seizures for 18 years concomitant to the discovery of high blood pressure. Initial scalp electroencephalography (EEG) showed seizure’s activity arising from the right temporal area. A noninjected cerebral computed tomography (CT) scan was then performed without abnormality. It was then treated as vascular epilepsy by vaproic acid. The drug resistance of this epilepsy motivated cerebral angiography. The neurological examination was normal. Cerebral angiography revealed an aneurysm of the right middle meningeal artery without any other intraparenchymal anomaly [
DISCUSSION
The aneurysm of the MMA is rare.[
CONCLUSIONS
Aneurysms of the middle meningeal artery are rare. Their mode of revelation by the seizures is unusual. The factors of rupture are not known. They are often posttraumatic or the consequence of perturbation of the cerebral circulation induced by other associated pathologies. When isolated, their physiopathology is identical to that of the aneurysms of the polygon of Willis. Their management uses the same techniques as for other cerebral aneurysms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bollati A, Galli G, Gandolfini M, Orlandini A, Gualandi GF. True aneurysm of the middle meningeal artery. Case report. J Neurosurg Sci. 1980. 24: 89-92
2. Bruneau M, Gustin T, Zekhnini K, Gilliard C. Traumatic false aneurysm of the middle meningeal artery causing an intracerebral hemorrhage: Case report and literature review. Surg Neurol. 2002. 57: 174-8
3. Cağavi F, Kalayci M, Unal A, Atasoy HT, Cağavi Z, Açikgöz B. Giant unruptured anterior communicating artery aneurysm presenting with seizure. J Clin Neurosci. 2006. 13: 390-4
4. Forbus WD. On the origin of miliary aneurysms of the superficial cerebral arteries. Bull Hopkins Hosp. 1930. 47: 239-84
5. Hänggi D, Winkler PA, Steiger H-J. Primary Epileptogenic Unruptured Intracranial Aneurysms: Incidence and Effect of Treatment on Epilepsy. Neurosurgery. 2010. 66: 1161-5
6. Hassler O. Medial defects in the meningeal arteries. J Neurosurg. 1962. 19: 337-40
7. Jussen D, Wiener E, Vajkoczy P, Horn P. Traumatic middle meningeal artery pseudoaneurysms: Diagnosis and endovascular treatment of two cases and review of the literature. Neuroradiology. 2012. 54: 1133-6
8. Kamali AW, Cockerell OC, Butlar P. Aneurysms and epilepsy: An increasingly recognised cause. Seizure. 2004. 13: 40-4
9. Kawaguchi T, Kawano T, Kaneko Y, Ooasa T, Ooigawa H, Ogasawara S. Traumatic lesions of the bilateral middle meningeal arteries—Case report. Neurol Med Chir (Tokyo). 2002. 42: 221-3
10. Kuba R, Krupa P, Okacova L, Rektor I. Unruptured intracranial aneurysm as a cause of focal epilepsy: An excellent postoperative outcome after intra-arterial treatment. Epileptic Disord. 2004. 6: 41-4
11. Miele VJ, Bendok BR, Batjer HH. Unruptured aneurysm of the middle cerebral artery presenting with psychomotor seizures: Case study and review of the literature. Epilepsy Behav. 2004. 5: 420-8
12. Sandin JA, Salamat MS, Baskaya M, Dempsey RJ. Intracerebral hemorrhage caused by the rupture of a nontraumatic middle meningeal artery aneurysm. Case report and review of the literature. J Neurosurg. 1999. 90: 951-4
13. Stehbens WE. Medial defects of the cerebral arteries of man. J Path Bact. 1959. 78: 179-85
14. Tsutsumi M, Kazekawa K, Tanaka A, Ueno Y, Nomoto Y, Nii K. Traumatic middle meningeal artery pseudoaneurysm and subsequent fistula formation with the cavernous sinus: Case report. Surg Neurol. 2002. 58: 325-8
15. Ulahannan TJ. Epileptic seizures due to cerebral artery aneurysm. J R Soc Med. 1998. 91: 325-
16. Yacubian EM, Rosemberg S, da Silva HC, Jorge CL, de Oliveira E, de Assis LM. Intractable complex partial seizures associated with posterior cerebral artery giant aneurysm: A case report. Epilepsia. 1994. 35: 1317-20

