

- Department of Physical Medicine and Rehabilitation, Gaziosmanpasa Taksim Training and Research Hospital, Istanbul, Turkey
- Department of Neurosurgery, Subdivision of Neuroradiology, Istanbul University Cerrahpasa Medical Faculty, Istanbul, Turkey
- Department of Radiology, Subdivision of Neuroradiology, Istanbul University Cerrahpasa Medical Faculty, Istanbul, Turkey
- Department of Physical Medicine and Rehabilitation, Istanbul Physical Medicine and Rehabilitation Training and Research Hospital, Istanbul, Turkey
Correspondence Address:
Rahsan Kemerdere
Department of Neurosurgery, Subdivision of Neuroradiology, Istanbul University Cerrahpasa Medical Faculty, Istanbul, Turkey
DOI:10.4103/sni.sni_405_17
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Belgin Erhan, Rahsan Kemerdere, Osman Kizilkilic, Berrin Gunduz, Murat Hanci. Acute tetraplegia following laryngotracheal reconstruction surgery. 16-Jan-2018;9:11
How to cite this URL: Belgin Erhan, Rahsan Kemerdere, Osman Kizilkilic, Berrin Gunduz, Murat Hanci. Acute tetraplegia following laryngotracheal reconstruction surgery. 16-Jan-2018;9:11. Available from: http://surgicalneurologyint.com/surgicalint-articles/acute-tetraplegia-following-laryngotracheal-reconstruction-surgery/
Date of Submission
30-Oct-2017
Date of Acceptance
24-Nov-2017
Date of Web Publication
16-Jan-2018
Abstract
Background:Paraplegia following thoracic spinal surgery or abdominal operations is usually attributed to spinal cord ischemia due to interruption of the segmental spinal vascular supply. Alternatively, the etiology of spinal cord ischemia following cervical surgery is less clear.
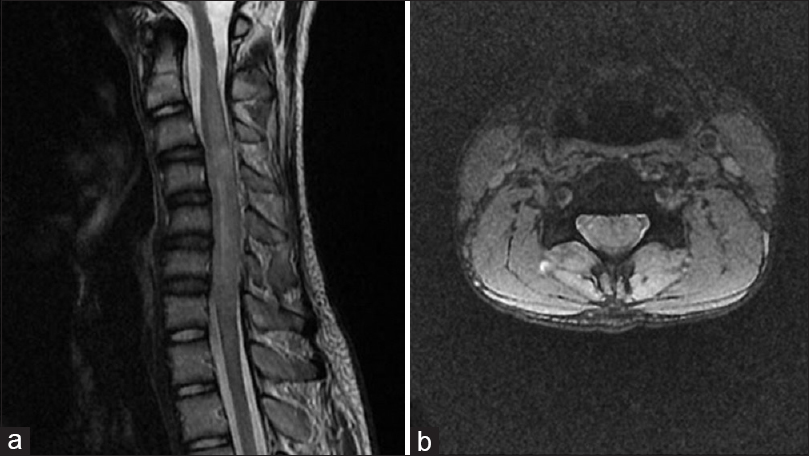
Case Description:A 14-year-old male became acutely tetraplegic with a C4 sensory level and sphincteric dysfunction 12 h following surgery for tracheal stenosis due to prior intubation. Signs included loss of pain and temperature below the level of C4 with preservation of deep sensations (position and vibration) and mute plantar responses. The cervical magnetic resonance imaging revealed diffuse intramedullary cord swelling between C2-C7 and hyperintense signal changes in the anterior and posterior columns of the cord on T2-weighted images. Various etiologies for this finding included a cervical hyperextension or hyperflexion injury vs. anterior spinal artery syndrome.
Conclusions:Postoperative treatment of spinal cord ischemia attributed to cervical and thoracoabdominal surgery is largely ineffective in reversing major neurological deficits. Therefore, it is critical to prevent ischemia during these procedures by the avoidance of coagulopathies, anemia, hypotension, and hyperflexion/hyperextension maneuvers.
Keywords: Anterior spinal artery syndrome, cervical, spinal cord injury, tracheal surgery
INTRODUCTION
Cervical myelopathy and spinal cord injury may result from hyperflexion/hyperextension occurring during surgical positioning.[
CASE REPORT
A 14-year-old male became acutely tetraplegic 12 h following treatment for tracheal stenosis. Three months earlier, after treatment for a metatarsal fracture, he sustained a respiratory arrest for 30 min; this was attributed to a massive pulmonary embolism. He was hospitalized in the intensive care unit (ICU) for the next 2 months. After discharge, he suffered from tracheal stenosis requiring tracheal resection/reconstruction. His neurological status before surgery was normal except for 4/5 motor power in his left distal lower extremity. Within 12 h of surgery, he became acutely tetraplegic with a C4 sensory level. His neurological examination revealed dissociated sensory loss with preservation of deep sensations (position and vibration). Anal tone was absent and plantar responses were mute.
Diagnostic studies
The T2-weighted cervical magnetic resonance imaging revealed a diffuse hyperintense signal, with accompanying diffuse cord swelling from C2-C7 [

DISCUSSION
The ASAS is largely attributed to vascular compromise to the spinal cord due to systemic hypotension, particularly in elderly patients.[
The diagnosis of ASAS is generally based on clinical findings. Compromise of anterior spinal artery results in upper motor neuron signs (flaccid paralysis, areflexia), loss of pain and temperature sensation, bladder and bowel dysfunction.[
Spinal cord infarction is usually due to occlusion of segmental vessels rather than direct involvement of anterior spinal artery. Here, a hyperextension injury, episodic hypotension, or a direct injury to branches from the vertebral arteries during tracheal reconstruction were all potential contributors to spinal cord ischemia.[
Treatment and prevention options for spinal cord ischemia
Paraplegia/tetraplegia due to spinal cord ischemia with no compressive etiology is not likely to recover. However, some strategies developed to protect the spinal cord from injury occurring during thoracic spinal and/or thoracoabdominal surgery include deep hypothermia, maintaining mean arterial blood pressure on the upper limit of normal, and cerebrospinal fluid drainage.[
CONCLUSION
While the thoracic spinal cord is more susceptible to vascular ischemia/events following spinal or abdominal surgery, it can occur postoperatively in the cervical region as well. Because postoperative treatments are ineffective, measures to prevent spinal cord ischemia should include avoiding systemic hypotension, anemia, hyperextension/hyperflexion during positioning, and inadvertent vascular dissection.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Augoustides JG, Stone ME, Drenger B. Novel approaches to spinal cord protection during thoracoabdominal aortic interventions. Curr Opin Anaesthesiol. 2014. 27: 98-105
2. Blacker DJ, Wijdicks EF, Ramakrishna G. Resolution of severe paraplegia due to aortic dissection after CSF drainage. Neurology. 2003. 61: 142-3
3. Cheshire WP, Santos CC, Massey EW, Howard JF. Spinal cord infarction: Etiology and outcome. Neurology. 1996. 47: 321-30
4. De Tommaso O, Caporuscio A, Tagariello V. Neurological complications following central neuraxial blocks: Are there predictive factors?. Eur J Anaesthesiol. 2002. 19: 705-16
5. Drummond JC, Lee RR, Owens EL. Spinal cord ischemia occurring in association with induced hypotension for colonic surgery. Anesth Analg. 2012. 114: 1297-300
6. Hobai IA, Bittner EA, Grecu L. Perioperative spinal cord infarction in nonaortic surgery: Report of three cases and review of the literature. J Clin Anesth. 2008. 20: 307-12
7. Hurlbert RJ. Strategies of medical intervention in the management of acute spinal cord injury. Spine. 2006. 31: S16-21
8. Johnson MH, Thorisso HM, DiLuna ML. Vascular Anatomy: The Head, Neck, and Skull Base. Neurosurg Clin N Am. 2009. 20: 239-58
9. Martínez-Lage JF, Almagro MJ, Izura V, Serrano C, Ruiz-Espejo AM, Sánchez-Del-Rincón I. Cervical spinal cord infarction after posterior fossa surgery: A case-based update. Childs Nerv Syst. 2009. 25: 1541-6
10. Ortega R, Suzuki S, Sekhar P, Stram JR, Rengasamy SK. Paraplegia after mastoidectomy under general anesthesia. Am J Otolaryngol. 2009. 30: 340-2
11. Weinberg L, Harvey WR, Marshall RJ. Post-operative paraplegia following spinal cord infarction. Acta Anaesthesiol Scand. 2002. 46: 469-72

