

- Department of Neurosurgery, David Geffen School of Medicine at UCLA, Los Angeles, California, USA
- Department of Neurosurgery, Kaiser Permanente Medical Center, Los Angeles, California, USA
Correspondence Address:
Daniel Diaz-Aguilar
Department of Neurosurgery, Kaiser Permanente Medical Center, Los Angeles, California, USA
DOI:10.4103/sni.sni_224_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Daniel Diaz-Aguilar, Sergei Terterov, Rudi Scharnweber, Catherine Merna, Stephanie Wang, Shayan Rahman. Adult sacrococcygeal teratoma with coccygectomy: A case report with a review of the literature. 24-Oct-2017;8:260
How to cite this URL: Daniel Diaz-Aguilar, Sergei Terterov, Rudi Scharnweber, Catherine Merna, Stephanie Wang, Shayan Rahman. Adult sacrococcygeal teratoma with coccygectomy: A case report with a review of the literature. 24-Oct-2017;8:260. Available from: http://surgicalneurologyint.com/surgicalint-articles/adult-sacrococcygeal-teratoma-with-coccygectomy-a-case-report-with-a-review-of-the-literature/
Date of Submission
20-Jun-2017
Date of Acceptance
15-Aug-2017
Date of Web Publication
24-Oct-2017
Abstract
Background:Saccrococcygeal teratomas (SCT) are derived from embryonic germ cell layers. They frequently present at the base of the coccyx within the pelvis. While these tumors are common in children, they are exceedingly rare in adults. In adults, a majority of these tumors are intrapelvic and associated with a low risk of malignant transformation. Therefore, this contributes to a good prognosis following resection of mostly benign lesions.
Case Description:An adult female with chronic pelvic pain presented with a sacral teratoma. She failed conservative treatment and underwent a coccygectomy with an en-bloc excision of the tumor. Microscopic histological analysis showed no evidence of immature or malignant elements, confirming the diagnosis of a mature, benign, cystic SCT.
Conclusions:Mature SCTs in adults are rare malignant lesions. In this case, the patient was cured following primary surgical excision requiring en-bloc coccygectomy.
Keywords: Adult, mature teratoma, sacral coccygectomy
INTRODUCTION
Sacrococcygeal teratomas (SCT) are multipotential cell tumors most commonly seen in neonates but only rarely in adults. SCTs carry a female preponderance of 4:1, and a prevalence of 1:30,000 births.[
CASE DESCRIPTION
Clinical presentation
A 23-year-old female presented with pelvic pain. Magnetic resonance imaging (MRI) of the pelvis revealed a complex cystic structure anterior to the coccyx [
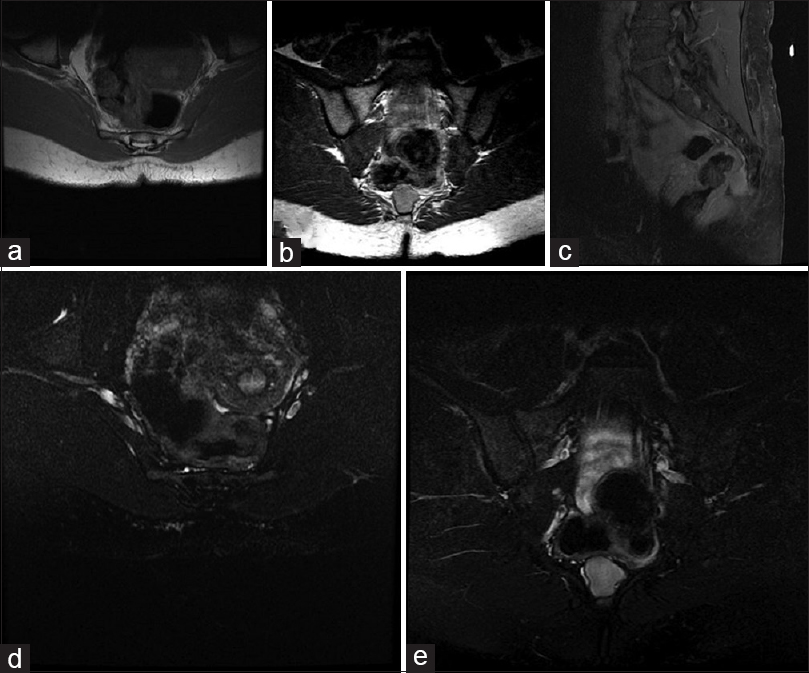
Figure 1
Axial T1-weighted (a), T2-weighted fat-saturated (b), sagittal T1-weighted post-gadolinium fat-saturated (c), coronal T1-weighted (d), and T2 fat-saturated (e) images demonstrating a complex precoccygeal cystic structure with multiple septations and fluid content of different signals and fluid levels
Surgery
The patient underwent an en-bloc posterior coccygectomy. Following exposure of the coccyx and lower part of the sacrum, the rectum was carefully dissected away from the tumor. An osteotome cut through the coccyx 6 cm above the tip [
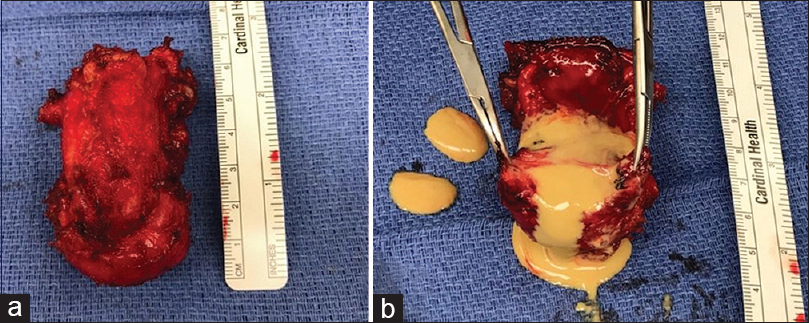
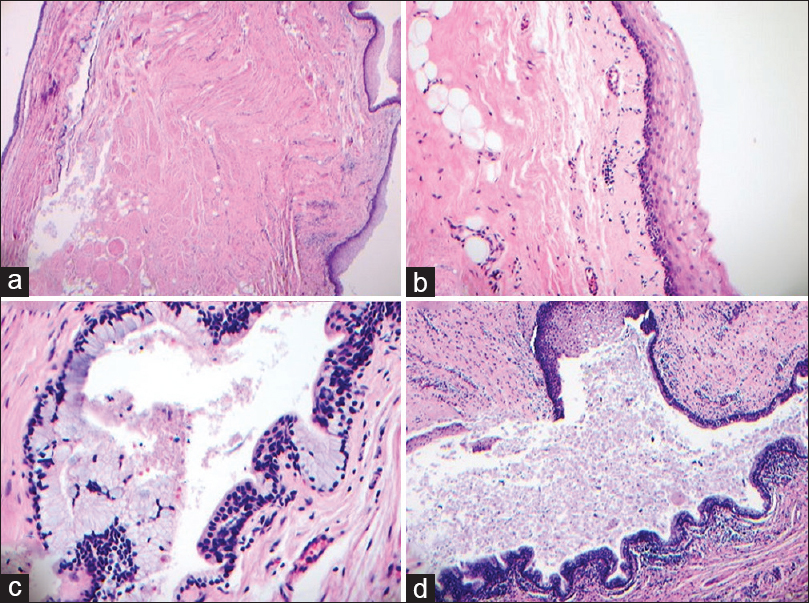
Figure 4
Histology of the mass demonstrating various types of mature tissue elements including lobules of smooth muscle, adipose tissue, stratified squamous epithelium (a, H and E, ×4; b, H and E, ×20) respiratory type ciliated epithelium (c, H and E, ×40; and mucous glandular tissue adjacent to stratified squamous epithelium (d, H and E, ×10)
DISCUSSION
Incidence and symptoms of sacrococcygeal teratoma
SCT are the most common fetal neoplasm. They account for 50% of teratomas in children but are rarely seen in adults.[
Sacrococcygeal teratoma characteristics in adults
SCTs are divided into Types I–IV (criteria proposed by Altman et al.) [
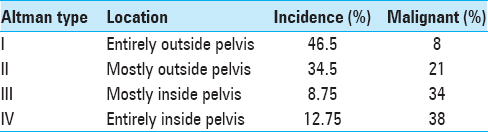
Table 1
Classification of sacrococcygeal teratomas[
Histopathology and use of markers
Mature SCT can be distinguished from immature teratomas by the presence of epithelial structures along with well-distinguished cartilage and muscular tissue. Immature teratomas contain primitive combinations of germ layers with occasional mature elements.[
Predominance
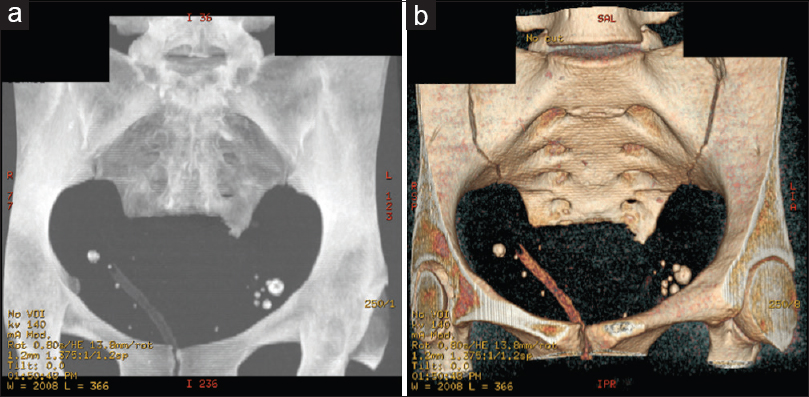
Computed tomography and MRI are both vital preoperative diagnostic studies for the visualization of a SCT.[
CONCLUSION
SCT, rarely observed in adults, are frequently benign, slowly growing intrapelvic masses best seen on MR studies. Mature benign SCT are highly susceptible to complete and early excision, without the additional need for chemotherapy or radiation.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Al-Essa A-A, Malik TA, Baghdadi MK, Tayeb El AA. Adult sacrococcygeal teratomas. Saudi Med J. 2004. 25: 367-9
2. Allsopp G, Sgouros S, Barber P, Walsh AR. Spinal teratoma: Is there a place for adjuvant treatment? Two cases and a review of the literature. Br J Neurosurg. 2000. 14: 482-8
3. Altman RP, Randolph JG, Lilly JR. Sacrococcygeal teratoma: American Academy of Pediatrics Surgical Section Survey-1973. J Pediatr Surg. 1974. 9: 389-98
4. Audet IM, Goldhahn RT, Dent TL. Adult sacrococcygeal teratomas. Am Surg. 2000. 66: 61-5
5. Bruneton JN, Diard F, Drouillard JP, Sabatier JC, Tavernier JF. Primary retroperitoneal teratoma in adults: Presentation of two cases and review of the literature. Radiology. 1980. 134: 613-6
6. Miles RM, Stewart GS. Sacrococcygeal teratomas in adult. Ann Surg. 1974. 179: 676-83
7. Panageas E. General diagnosis case of the day. Primary retroperitoneal teratoma. AJR Am J Roentgenol. 1991. 156: 1292-4

