

- Professor of Clinical Neurosurgery, School of Medicine, State University of New York at Stony Brook, New York , and Chief of Neurosurgical Spine and Education, NYU Winthrop Hospital, NYU Winthrop NeuroScience/Neurosurgery, Mineola, New York 11501, United States.
DOI:10.25259/SNI_423_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nancy E. Epstein. Case of the Week: Preoperative MR/CT Diagnosis of Left L2-L3 Disc Surgically Documented As Massive Synovial Cyst. 30-Aug-2019;10:168
How to cite this URL: Nancy E. Epstein. Case of the Week: Preoperative MR/CT Diagnosis of Left L2-L3 Disc Surgically Documented As Massive Synovial Cyst. 30-Aug-2019;10:168. Available from: http://surgicalneurologyint.com/surgicalint-articles/case-of-the-week-preoperative-mr-ct-diagnosis-of-left-l2-l3-disc-surgically-documented-as-massive-synovial-cyst/
Date of Submission
18-Jul-2019
Date of Acceptance
19-Jul-2019
Date of Web Publication
30-Aug-2019
Abstract
Background: The diagnosis of a lumbar herniated disc, stenosis, and other degenerative findings are typically established preoperatively with MR scans, supplemented with non-contrast CT studies. Here, a 77-year-old female, diagnosed as having L2-S1 stenosis and a large left-sided L2-L3 herniated disc was found at surgery to have a massive left-sided L2-L3 synovial cyst.
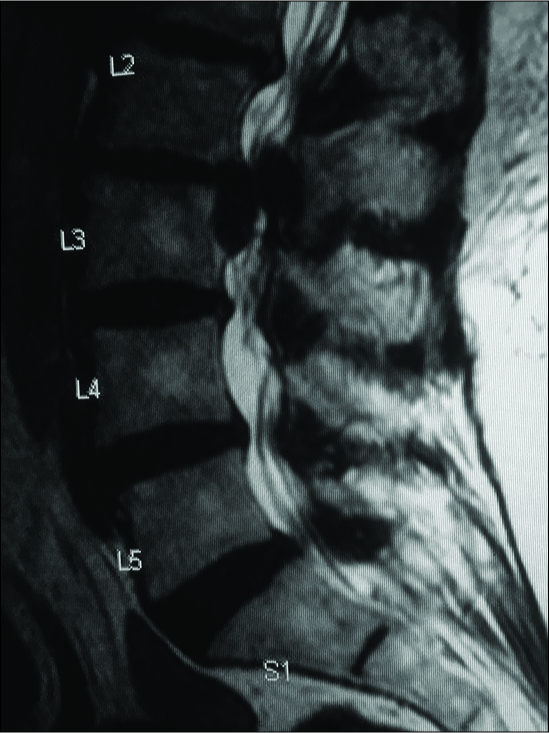
Case Description: A 77-year-old female was followed by pain management for 6-months with proximal left lower extremity weakness. The lumbar MR at that time was read as demonstrating a large left L2-L3 disc herniation with inferior migration to the L3 mid pedicle level, accompanied by L2-S1 lumbar stenosis. When she finally consulted neurosurgery, she exhibited severe left iliopsoas and quadriceps weakness (2/5), absent lower extremity reflexes, and profound decreased pin appreciation in the left L2-L3 distributions. The repeat MR and new CT studies confimred a large left L2-L3 disc accompanied by moderate/marked L2-S1 stenosis. However, at surgery, consisting of a laminectomy L2-S1, the supposed left L2-L3 disc proved to be a massive synovial cyst. Postoperatively, the patient regained normal function, and remained neurologically intact 6 months later.
Conclusion: In this 77 year-old female, the preoperative MR and CT scans were interpreted as showing a “typical” large left L2-L3 herniated disc. This proved at surgery to be a massive left L2-L3 synovial cyst. As demonstrated in this case, older patients with degenerative lumbar disease/stenosis, may have synovial cysts that mimic disc herniations both clinically and on preoperative diagnostic studies.
Keywords: Lumbar Disc, Synovial Cyst, Stenosis, MR, CT Diagnosis
INTRODUCTION
Prior to surgery, lumbar herniated discs are frequently diagnosed on MR/CT studies as accompanying spinal stenosis. Here, a 77-year-old female with the classical preoperative diagnosis of a left-sided L2-L3 herniated disc accompanied by L2-S1 lumbar stenosis was found at surgery to have a massive left L2-L3 synovial cyst. In older patients, there should be a greater anticipation that synovial cysts rather than disc herniations may accompany degenerative lumbar disease/stenosis.
CASE
A 77-year-old female, followed by pain management, presented with 6 months of proximal left lower extremity pain, weakness, and numbness. The 6-month old MR demonstrated significant lumbar stenosis L2-S1, and was interpreted as showing a large left L2-L3 disc herniation with marked inferior migration to the left L3 mid-pedicular level. Two months prior to presentation, she had undergone two epidural steroid injections. When she was finally seen by neurosurgery, she had significant left iliopsoas/quadriceps weakness (2/5), absent lower extremity reflexes, and profound pin loss in the left L2-L3 distrubutions. The follow-up MR and new CT studies were similarly interpreted as showing L2- S1 stenosis and a left-sided L2-L3 disc. However, when she underwent a L2-S1 laminectomy, the left L2-L3 lesion proved to be a massive synovial cyst [

DISCUSSION
Etiology and Location of Synovial Cysts
In 2004, Epstein noted synovial cysts occur as the result of arthrotic disruption of the facet joint. With degenerative spondylolisthesis, (DS), synovial cysts may occur in up to 40% of cases.[
Myth of Successful Synovial Cyst Aspiration
Synovial cysts are typically tough, firm, and tenacious, with large fibrous capsules adherent to surrounding dura/nerve roots. They contain just small amounts of gelatinous tissue and/or thick crank-case fluid. It is, therefore, no surprise that multiple studies reviewed in 2012 by Epstein and Baisden documented a 50-100% failure rate for attempts at percutaneously aspirating these lesions by “pain management specialists” under fluoroscopic or CT-guidance. Rather, surgical excision results in excellent resolution of back and radicular pain (e.g. 91.6-92.5% and 91.1-91.9% recovery respectively).[
Efficacy of Laminectomy Alone for Treatment of Lumbar Synovial Cysts
Multiple studies have documented the efficacy of laminectomy alone for the treatment of lumbar synovial cysts, without the need for fusion. Siu and Stoodley (2018) advocated laminectomy alone for 46 patients with lumbar synovial cysts who were followed an average of 43 mos. (1 month-13 years); only 2 (4.3%) later required fusions.[
Few MR Studies Misdiagnose Lumbar Discs As Synovial Cysts or Tumors
Few MR studies have misdiagnosed lumbar disc herniations as synovial cysts or tumors. In 2010, Teufack et al. treated a 49-year-old male whose enhanced MR scan showed a dorsolateral peripherally enhancing epidural lesion resulting in marked dural compression.[
CONCLUSION
On rare occasion, lumbar synovial cysts may mimic herniated lumbar discs that have extruded dorsolaterally [
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alfonso MA, Sierra MO, Del Corral GSOL, Lopez VAJ, Gonzalez-Quarante LH, Vendrell SE. Misdiagnosis of posterior suquestrated lumbar disc herniation: report of three cases and review of the literature. Spinal Cord Se Cases. 2018. 4: 61-
2. Epstein NE. Lumbar synovial cysts: a review of diagnosis, surgical management, and outcome assessment. J Spinal Disord Tech. 2004. 17: 321-5
3. Epstein NE, Baisden J. The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surg Neurol Int. 2012. 3: S157-66
4. Epstein NE.editorsSpinal case of the month with short perspective: How would you treat this L3-L4 synovial cyst? Surg Neurol Int. 2018. 9: 56-
5. Hohenberger C, Brawanski A, Ullrich OW, Höhne J, Zeman F, Schebesch KM. Degenerative symptomatic spinal synovial cysts: Clinical presentation and functional outcome. J Clin Neurosci. 2019. 62: 112-116
6. Siu KC, Stoodley MA.editors. Decompressive laminectomy without fusion for lumbar facet joint cysts. J Clin Neurosci. 2018. 58: 113-116
7. Teufack SG, Singh H, Harrop J, Ratliff J. Dorsal epidural intervertebral disk herniation with atypical radiographic findings: case report and literature review. 2010. 33: 268-71

