

- Department of Neurosurgery, Showa University School of Medicine, Shinagawa, Tokyo, Japan
Correspondence Address:
Shintaro Arai
Department of Neurosurgery, Showa University School of Medicine, Shinagawa, Tokyo, Japan
DOI:10.25259/SNI-69-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Shintaro Arai, Katsuyoshi Shimizu, Tohru Mizutani. Chondroma in the hypoglossal canal: A case report. 24-Apr-2019;10:63
How to cite this URL: Shintaro Arai, Katsuyoshi Shimizu, Tohru Mizutani. Chondroma in the hypoglossal canal: A case report. 24-Apr-2019;10:63. Available from: http://surgicalneurologyint.com/surgicalint-articles/9291/
Date of Submission
29-Sep-2018
Date of Acceptance
27-Feb-2019
Date of Web Publication
24-Apr-2019
Abstract
Background:Intracranial chondromas are rare tumors arising from the skull base. They are usually accompanied by functional impairments of some cranial nerves. However, hypoglossal nerve dysfunction is rare.
Case Description:We report on a 57-year-old woman presenting with chondroma of the right hypoglossal canal leading to right hypoglossal nerve palsy.
Conclusions:This report suggests that chondroma should be considered as a differential diagnosis in cases of hypoglossal lesions.
Keywords: Chondroma, hypoglossal canal, hypoglossal nerve palsy, skull base
INTRODUCTION
Intracranial chondromas, rare tumors accounting for 0.1%–0.2% of all intracranial tumors,[
CASE REPORT
A 57-year-old woman presented with difficulty in swallowing that progressed over 6 months. No neurological deficits other than right hypoglossal nerve palsy were detected on physical examination. She had a history of successfully treated breast cancer. The patient provided informed consent.
Computed tomography (CT) revealed skull base erosion from the right hypoglossal canal to the anterior part of the foramen magnum [
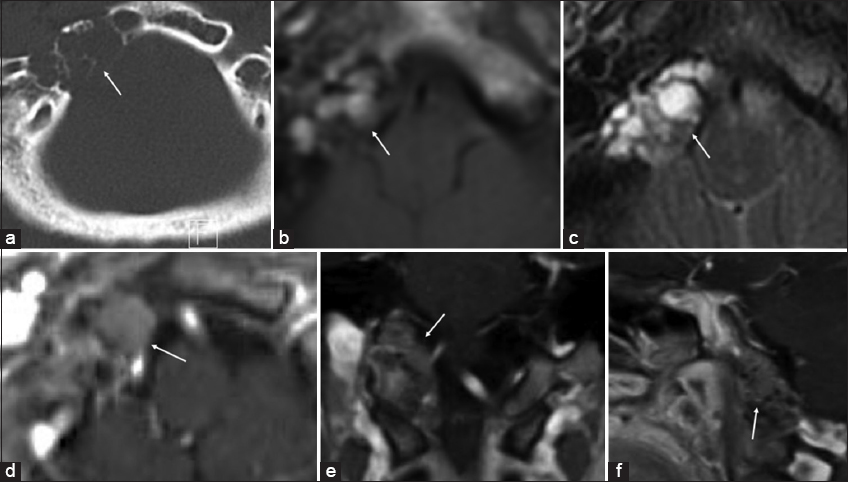
The patient underwent tumor removal through the transcondylar approach using image-guided navigation; a gray mass lesion was encountered in the hypoglossal canal, with part of the tumor progressing into the dura. Motor-evoked potentials of the hypoglossal nerve decreased during tumor debulking, resulting in the subtotal resection.
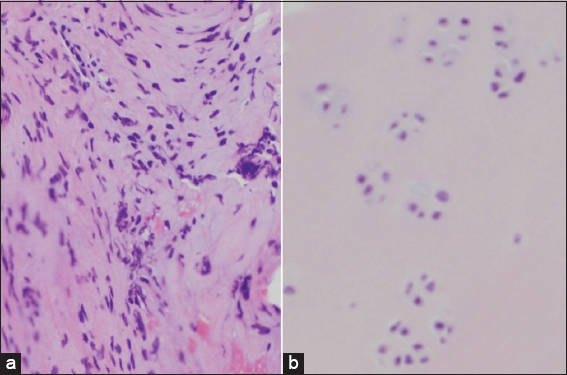
Microscopic examination revealed a cartilaginous hyaline matrix and well-differentiated regular shaped cells with a clear cytoplasmic halo [
Postoperatively, the patient had no complications and did not receive radiation therapy due to the absence of pathological malignancy. MRI showed no regrowth a year after surgery.
DISCUSSION
Intracranial chondromas, first reported by Hirshfield in 1851,[
The standard treatment for chondromas and chondrosarcomas is complete surgical removal. However, total resection is difficult due to the deep location of the tumor or invasion toward the cranial nerves and critical vascular structures. Postoperative radiation treatment is controversial,[
CONCLUSIONS
We reported a case of chondroma in the hypoglossal canal. For understanding prognosis and selecting treatment strategies, it is important to distinguish these from other diseases. Chondroma and chondrosarcoma should be considered as differential diagnoses of hypoglossal canal tumors. Furthermore, a partially resected chondroma should be followed-up even if it is benign.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that her name and initial will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alharbi FA, Lenarz T, Stoever T. A case of unilateral hypoglossus nerve palsy associated with chordoma in the region of clivus. Eur Arch Otorhinolaryngol. 2009. 266: 2001-3
2. Amichetti M, Amelio D, Cianchetti M, Enrici RM, Minniti G. A systematic review of proton therapy in the treatment of chondrosarcoma of the skull base. Neurosurg Rev. 2010. 33: 155-65
3. Cushing H.editorsIntracranial Tumors, Notes upon a Series of two Thousand Verified Cases with Surgical-Mortality Percentages Pertaining Thereto. Springfield Illinois: Charles C Thomas; 1932. p. 133-
4. De Coene B, Gilliard C, Grandin C, Nisolle JF, Trigaux JP, Lahdou JB. Unusual location of an intracranial chondroma. AJNR Am J Neuroradiol. 1997. 18: 573-5
5. Dutton J. Intracranial solitary chondroma. Case report. J Neurosurg. 1978. 49: 460-3
6. Higashida T, Sakata K, Kanno H, Tanabe Y, Kawasaki T, Yamamoto I. Intracranial chondroma arising from the skull base:Two case reports featuring the image findings for differential diagnosis. No Shinkei Geka. 2007. 35: 495-501
7. Hines JP, Howard BE, Hoxworth JM, Lal D. Positive and negative predictive value of PET-CT in skull base lesions:Case series and systematic literature review. J Neurol Surg Rep. 2016. 77: e39-45
8. Krishnan S, Foote RL, Brown PD, Pollock BE, Link MJ, Garces YI. Radiosurgery for cranial base chordomas and chondrosarcomas. Neurosurgery. 2005. 56: 777-84
9. Nakayama M, Nagayama T, Hirano H, Oyoshi T, Kuratsu J. Giant chondroma arising from the dura mater of the convexity. Case report and review of the literature. J Neurosurg. 2001. 94: 331-4
10. Patel A, Munthali L, Bodi I. Giant cystic intracranial chondroma of the falx with review of literature. Neuropathology. 2009. 29: 315-7
11. Weindling SM, Wood CP, Hoxworth JM. Hypoglossal canal lesions:Distinctive imaging features and simple diagnostic algorithm. AJR Am J Roentgenol. 2017. 209: 1119-27
12. Weng JC, Li D, Li H, Ma JP, Tian KB, Wang L. Surgical management and outcomes of intracranial chondromas:A single-center case series of 66 patients. World Neurosurg. 2017. 108: 264-77

