

- Department of Neurosurgery, Saiseikai Shiga Hospital, Imperial Gift Foundation Inc., Ritto, Shiga, Japan
Correspondence Address:
Shigeomi Yokoya
Department of Neurosurgery, Saiseikai Shiga Hospital, Imperial Gift Foundation Inc., Ritto, Shiga, Japan
DOI:10.4103/sni.sni_152_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Shigeomi Yokoya, Akihiko Hino, Hideki Oka. Chronic headache caused by a titanium fixation plate: Report of two cases. 26-Sep-2017;8:238
How to cite this URL: Shigeomi Yokoya, Akihiko Hino, Hideki Oka. Chronic headache caused by a titanium fixation plate: Report of two cases. 26-Sep-2017;8:238. Available from: http://surgicalneurologyint.com/surgicalint-articles/chronic-headache-caused-by-a-titanium-fixation-plate-report-of-two-cases/
Date of Submission
28-Apr-2017
Date of Acceptance
29-Jul-2017
Date of Web Publication
26-Sep-2017
Abstract
Background:We report two patients with chronic postcraniotomy headache who showed rapid alleviation of pain after removal of titanium miniplates.
Case Description:(Case 1) A 26-year-old woman underwent a right frontal craniotomy and excision of the entire cerebral cavernous malformation. Eleven years later, she developed headache. The titanium plate was removed and the patient presented complete amelioration of headache. (Case 2) A 50-year-old man underwent an aneurysm clipping via the lateral supraorbital approach of the left side. One year later, he complained about throbbing pain. Removing the titanium plate led to complete relief of the headache.
Conclusion:Titanium miniplate fixation may irritate the deep division of the supraorbital nerve and may cause a chronic headache. Here, we propound the idea that, postcraniotomy, titanium miniplates should not be placed above the temporal fusion line.
Keywords: Postcraniotomy headache, supraorbital nerve, temporal fusion line, titanium miniplates
BACKGROUND
Titanium miniplates have been used for decades as a standard postoperative procedure for the fixation of bone flaps after craniotomy. They provide easy, rigid, and long-lasting fixation. However, a small but significant number of complications have been reported including skin irritation,[
CASE REPORTS
Case 1
A 26-year-old, previously healthy woman experienced headache, vomiting, and left hemiparesis in August 2002. Computed tomography (CT) scanning and magnetic resonance (MR) imaging revealed a probable cerebral cavernous malformation (CCM). She underwent a right frontal craniotomy and an excision of the entire CCM. She was discharged with no neurological complication or headache. In January 2013, she developed progressive dull headache on the right side, and physical examination revealed local tenderness just above the titanium miniplate [
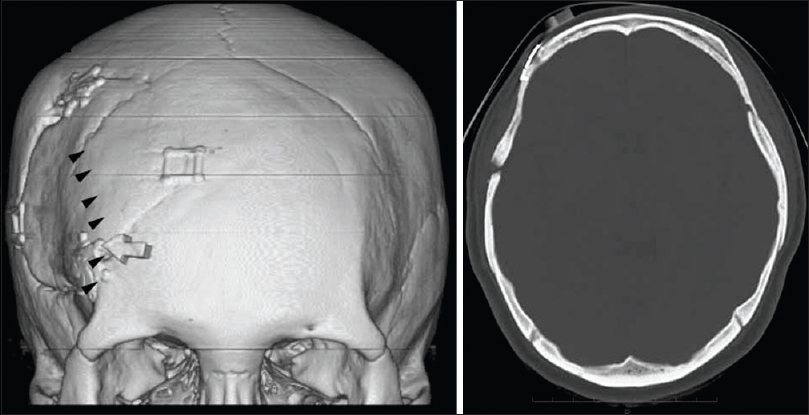
Figure 1
Preoperative 3-D computed tomography (3D-CT) images (left) and skull windows for the migration of the titanium hardware, on axial CT image (right) for the patient in case 1. Arrow indicates the location marked using a plastic eraser and denotes the oppressive point of the scalp and arrowheads indicate the position of the temporal fusion line. The titanium miniplate was placed above the temporal fusion line
Case 2
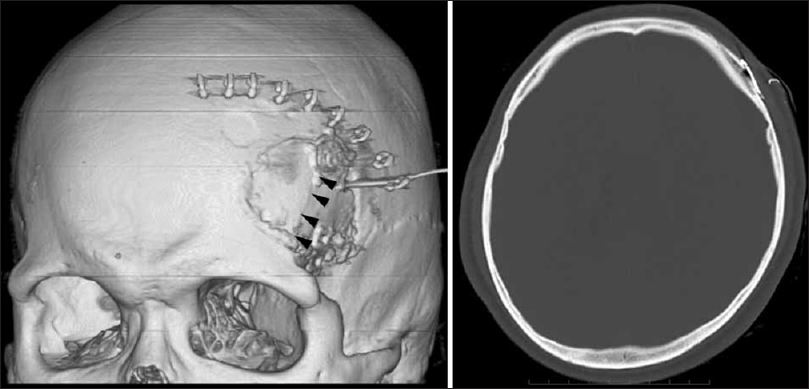
A 50-year-old man with an unremarkable history developed subarachnoid hemorrhage (SAH) caused by rupture of a saccular aneurysm at the bifurcation of the left internal carotid artery and the posterior communicating artery in April 2014. He underwent an aneurysm clipping via the lateral supraorbital (LSO) approach of the left side and returned to normal life without any neurological deficits; although he felt a mild headache upon discharge from the hospital. In the summer of 2015, he complained of throbbing pain localized to the left forehead. Pressure pain was recorded in the left forehead immediately above the titanium miniplate [
DISCUSSION
Kaur et al. reported that fifteen of the 126 consecutive patients (11.9%) who underwent supratentorial craniotomy, had constant headaches one year after surgery.[
A detailed mechanism of the cause of the pain is still unknown. However, it is proposed that the metal plate may directly irritate the sensory nerve or cause an allergic reaction, which may produce local inflammation. However, in our cases, it is reasonable to consider that the titanium miniplate fixation caused irritation of the peripheral nerve of the scalp since both of our patients experienced pressure pain immediately above the plate and were relieved of the postcraniotomy headache by plate removal. The characteristics of pain observed in our patients correspond to those of nociceptive pain, i.e., progressive, long lasting, unilateral, and dull frontal headache with local tenderness just above the miniplate.
It is noteworthy that in both the cases, the titanium miniplate was placed right above the temporal fusion line [Figures
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Beck J, Parent A, Angel MF. Chronic headache as a sequela of rigid fixation for craniosynostosis. J Craniofac Surg. 2002. 13: 327-30
2. de Gray LC, Matta BF. Acute and chronic pain following craniotomy: A review. Anaesthesia. 2005. 60: 693-704
3. Kaur A, Selwa L, Fromes G, Ross DA. Persistent headache after supratentorial craniotomy. Neurosurgery. 2000. 47: 633-6
4. Knize DM. A study of the supraorbital nerve. Plast Reconstr Surg. 1995. 96: 564-9
5. Noda K, Tanikawa R, Sugimura T, Kawasaki K, Kimura T, Izumi N. Use of bioabsorbable plates for cranial fixation. Neurol Med Chir. 2009. 49: 559-62
6. Shimizu S. Scalp neuralgia and headache elicited by cranial superficial anatomical causes: Supraorbital neuralgia, occipital neuralgia, and post-craniotomy headache. Clin Neurol. 2014. 54: 387-94
7. Spetzler RF. Bone flap fixation: A new technique: Technical note. J Neurosurg. 1997. 87: 475-6
8. Takahashi N, Fujiwara K, Saito K, Tominaga T. Interdigitated craniotomy: A simple technique to fix a bone flap with only a single plate. J Neurosurg. 2015. 123: 1055-8
9. Wakui D, Nagashima G, Ueda T, Takada T, Tanaka Y, Hashimoto T. Three cases of scalp rupture and cosmetic deformity caused by a fixation plate after craniotomy. Jpn J Neurosurg (Tokyo). 2012. 21: 138-42


Nicole Contreras
Posted April 8, 2020, 2:44 pm
I had a tumor removed from the left frontal lobe of my brain. I was an approximate size of a golf ball. Since my procedure in March of 2020 I have had excruciating headaches that can vary in intensity but are always present. In the last week or two things have gotten worse. I have de eloped a stuttering problem that has been progressively getting much worse. Im getting beyond words to describe the pain and frustration I’m experiencing due to both these issues, and besides that I have also developed evening nauseas. Medication is not eliminating any of my symptoms
Ladybug
Posted November 10, 2021, 3:59 pm
I am now a 54-year-old Caucasian female. Diagnosed with a right temporal optic sheath meningioma, January 18th/2018 my meningioma the size of a golf ball was also removed. Immediate temporal and job pain that is never left me. I have been able to feel the titanium screws since the inflammation went down. I know feel even more screws and even more excruciating pain and constant hemiplegia headaches. What more can I say .. except, I wish not this on anyone.