

- Department of Neurosurgery, Aga Khan University Hospital, Karachi, Pakistan
- Department of Pathology, Aga Khan University Hospital, Karachi, Pakistan
Correspondence Address:
Asra Tanwir
Department of Pathology, Aga Khan University Hospital, Karachi, Pakistan
DOI:10.4103/sni.sni_246_18
Copyright: © 2019 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Asra Tanwir, Noor Malik, Gohar Javed, Romana Idrees. Dermoid cyst with no intracranial extension: A case report and literature review. 28-Feb-2019;10:25
How to cite this URL: Asra Tanwir, Noor Malik, Gohar Javed, Romana Idrees. Dermoid cyst with no intracranial extension: A case report and literature review. 28-Feb-2019;10:25. Available from: http://surgicalneurologyint.com/surgicalint-articles/9210/
Date of Submission
17-Jul-2018
Date of Acceptance
19-Nov-2018
Date of Web Publication
28-Feb-2019
Abstract
Background:Dermoid cysts are cystic inclusion tumors. They comprise hair follicles, sweat glands, and sebaceous glands. They have lining of stratified squamous epithelium. The most common areas involved are face, lower back, and ovaries. Congenital cystic dermoid involving the anterior fontanelle with no intracranial extension is a rare scalp swelling. We present a case of dermoid cyst with no intracranial extension.
Case Description:We report a case of 4-month-old child presented with a history of a scalp swelling since birth. The swelling increased in size progressively. Magnetic resonance imaging of the brain revealed extracranial cystic lesion over anterior fontanelle with no intracranial extension. Cyst was excised completely with no postoperative complications. On histopathology it was dermoid cyst.
Conclusion:To the best of our knowledge, congenital dermoid cyst of the anterior fontanelles is rare. Complete surgical excision is the treatment of choice.
Keywords: Anterior fontanelle, cyst, dermoid, scalp
INTRODUCTION
Dermoid cyst is a benign, slowly growing lesion that accounts for 0.1–0.5% of all intracranial lesions.[
CASE HISTORY
A 4-month old girl was brought by her parents with complain of scalp swelling over anterior Fontanelle since birth. The swelling gradually increased in size. On examination, there was a soft, fluid-filled lesion over the anterior fontanelle, which was nontender and nonpulsatile. Trans illumination test and cough impulse were negative. There was no bruit over the swelling. Magnetic resonance imaging of brain was carried out, which revealed presence of a well-defined cystic swelling in the midline over the anterior fontanelle, measuring approximately 35 × 30 × 18 mm in transverse, anterior-posterior, and craniocaudal dimensions. It was cystic in appearance, with hyperintense signals on T2-weighted sequence, with no flow voids [
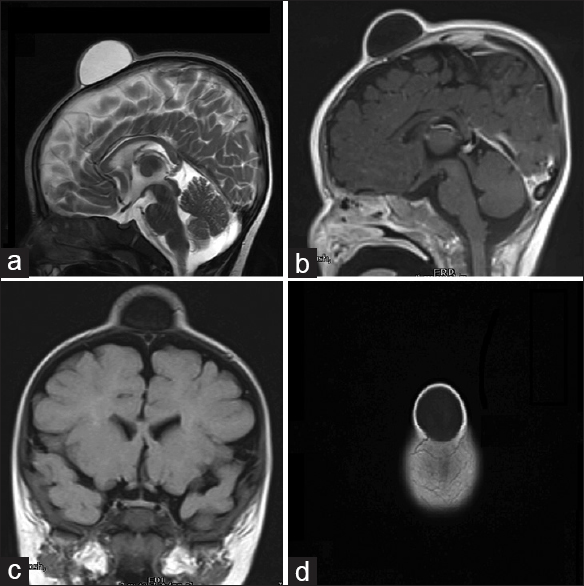
No immature components such as hair or teeth were found within the lesion. Features were consistent with dermoid cyst.
DISCUSSION
Congenital inclusion dermoid cysts are thought to arise during the third and fifth week of embryogenesis from displacement of germ cells.[
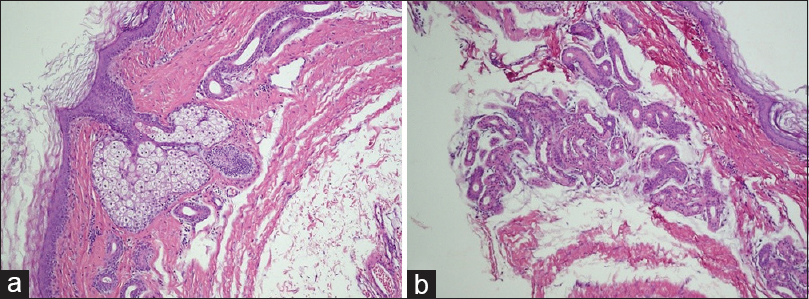
On histopathological examination, dermoid cyst consists of keratinizing stratified squamous epithelial lining, with some adnexal appendage structure-like intraluminal keratin and most commonly sebaceous glands.[
Imaging is important postoperatively to monitor the status of these patients. In our patient no recurrence has been noticed after 6 weeks of surgery.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Agrawal A, Santhi V, Reddy V. Subgaleal dermoid cyst of the anterior fontanelle in a child. Egypt J Radiol Nucl Med. 2015. 46: 1171-4
2. Crawford R. Dermoid cyst of the scalp: Intracranial extension. J Pediatr Surg. 1990. 25: 294-5
3. De Carvalho GT, Fagundes-Pereyra WJ, Marques JA, Dantas FL, de Sousa AA. Congenital inclusion cysts of the anterior fontanelle. Surg Neurol. 2001. 56: 400-5
4. Iwamuro Y, Shirahata M, Jito J, Tokime T, Hosotani K, Tokuriku Y. A case report of a scalp dermoid cyst containing watery-clear fluid. No Shinkei Geka. 2002. 30: 211-4
5. Kumar S, Singh M, Agarwal P. Giant congenital dermoid cyst of scalp. J Cran Max Dis. 2014. 3: 147-9
6. Lebkowski WJ, Lebkowska U, Dzieciol J. The giant dermoid cyst of the scalp mimicking skull tumor. Case report. Rocz Akad Med Bialymst. 2000. 45: 47-53
7. Liu JK, Gottfried ON, Salzman KL, Schmidt RH, Couldwell WT. Ruptured intracranial dermoid cysts: Clinical, radiographic, and surgical features. Neurosurgery. 2008. 62: 377-84
8. Makhija D, Sisodiya N, Shah H, Waghmare M. Cystic congenital scalp inclusion dermoid: A case report. Dev Period Med. 2016. 20: 287-8
9. Reissis D, Pfaff MJ, Patel A, Steinbacher DM. Craniofacial dermoid cysts: Histological analysis and inter-site comparison. Yale J Biol Med. 2014. 87: 349-57
10. Stendel R1, Pietilä TA, Lehmann K, Kurth R, Suess O, Brock M. Ruptured intracranial dermoid cysts. Surg Neurol. 2002. 57: 391-8
11. Wax MK, Briant TD. Epidermoid cysts of the cranial bones. Head Neck. 1992. 14: 293-6
12. Yang JS, Choi HJ, Cho YJ, Kang SH. Sensory complications in patients after scalp mass excision and its anatomical considerations. J Korean Neurosurg Soc. 2014. 55: 200-4

