

- Neurointervencionismo, Hospital El Cruce, Florencio Varela, Buenos Aires,
- Neurocirugía, Hospital de Clinicas, UBA, Buenos Aires, Argentina,
- Radiología, Hospital Vithas Parque San Antonio, Málaga, España.
Correspondence Address:
Javier Goland
Neurocirugía, Hospital de Clinicas, UBA, Buenos Aires, Argentina,
DOI:10.25259/SNI_410_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Javier Goland, Luis Domitrovic, Gustavo Doroszuk, Silvia Garbugino, Paula Ypa. Distal radial approach for neurointerventional diagnosis and therapy. 01-Nov-2019;10:211
How to cite this URL: Javier Goland, Luis Domitrovic, Gustavo Doroszuk, Silvia Garbugino, Paula Ypa. Distal radial approach for neurointerventional diagnosis and therapy. 01-Nov-2019;10:211. Available from: http://surgicalneurologyint.com/surgicalint-articles/9733/
Date of Submission
26-Aug-2019
Date of Acceptance
09-Oct-2019
Date of Web Publication
01-Nov-2019
Abstract
Background: The transradial approach results in fewer complications at the puncture site, lower hospital costs, and greater comfort for patients. The distal transradial approach (dTRA) adds some benefits over the conventional radial approach. The objective is to describe initial experience with distal radial approach technique and the results obtained for neuroendovascular diagnostic and therapeutic procedures.
Methods: Description of distal radial approach technique and obtained data from the first 3 months experience using this approach as the first choice for neuroendovascular procedures in two neuroendovascular centers.
Results: Of the total of 94 procedures performed during 3 months, 67 were diagnostic and 27 were therapeutic. Eleven (16%) of the diagnostic procedures were performed through the dTRA. Of the 27 embolizations, eight (30%) were done using this approach. Every distal radial approach that was performed for diagnosis and therapeutics was successful.
Conclusion: Puncture of the radial artery within the anatomical snuffbox is a radial approach variation option for diagnostic and therapeutic neuroendovascular procedures.
Keywords: Approach, Distal radial, Neurointerventional
BACKGROUND
The transradial approach has emerged as a neurointerventional option for the diagnosis and treatment of cerebral aneurysms.[
There are some reports of cardiac catheterizations and cerebral angiographies performed through a more distal radial approach, alternatively called the distal transradial approach (dTRA), snuffbox approach, or very dTRA.[
The dTRA approach has some benefits with respect to the conventional radial approach. These include (1) that arterial puncture is performed distal to the deep palmar arch formation, which ensures permeability of the palmar arch after the procedure; (2) that the neutral hand position is more comfortable for both the awake patient and the operator; and (3) that the left distal radial artery is more comfortable for the operator to puncture than the left traditional transradial approach. Another reason relates to the floor of the anatomical snuffbox being formed by two carpal bones – the trapezium and scaphoid – that being rigid structures, facilitate compression for hemostasis. Furthermore, subcutaneous hematomas rarely spread from the wrist to the upper part of the forearm, and there is no need to compress the wrist for hemostasis, which makes the wrist free to move and thereby limits venous congestion of the hand. Moreover, if vasospasm occurs or a hematoma develops from unsuccessful needling, thereby rendering further distal attempts more difficult, an operator can easily move proximal to adopt the conventional radial approach. Finally, the snuffbox approach saves more undamaged length of the radial artery for potential extracranial-intracranial artery bypass surgery candidates.[
There are some disadvantages of this approach: (a) the artery has a smaller caliber, more tortuous, and more vulnerable to spam in the anatomical snuffbox and needling can be more difficult than the conventional approach, due to the tortuosity a floppy 0.018 or 0.014-inch guide wire may be required; (b) needling theoretically can cause pain by irritating radial nerve and periosteum but there are no reports of this complication yet; (c) the scant soft tissue around the snuffbox might not secure the sheath properly; (d) since radial artery is smaller in caliber in the snuffbox, sheaths larger than 6Fr are difficult to be introduced; and (e) since there are many anatomic variations below the wrist across patients, the snuffbox approach is not always feasible.[
The objective of this paper is to describe the distal radial approach technique and the results obtained using it over the first 3 months during which this approach was employed for neuroendovascular diagnostic and therapeutic cerebral procedures at two centers at which the conventional radial approach had already been used as the first option for 3 years. The current cohort of patients is compared against those from the previous 3 months and to the frequency of needing to resort to a femoral approach.
MATERIALS AND METHODS
On March 25, 2019, puncture of the radial artery at the level of the anatomical snuffbox began to be used within two neurointerventional services as the first option for diagnostic or therapeutic cerebrovascular procedures involving patients over 18 years of age.
Description of the technique: for diagnostic procedures, local anesthesia is used at the puncture site, while general anesthesia is used for all therapeutic procedures. The distal radial approach is the first approach option currently employed, with failures progressing to the radial artery in the forearm within the pulse channel and then in cases of continued failure, the femoral approach.
For the distal radial approach, the boundaries of the anatomic snuffbox and radial artery path are demarcated [




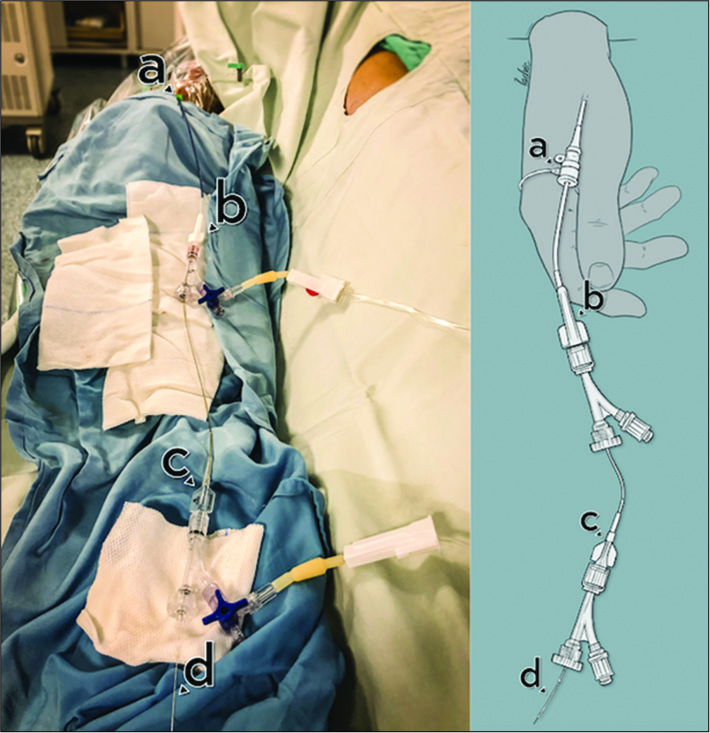
Figure 4:
The case in which bilateral approach was performed. Solid black arrow shows radial sheath inserted into the left radial artery through the snuffbox with the limb flexed and resting on the patient’s abdomen. Dotted arrow points out radial sheath inserted into the right radial artery through the classic transradial approach.
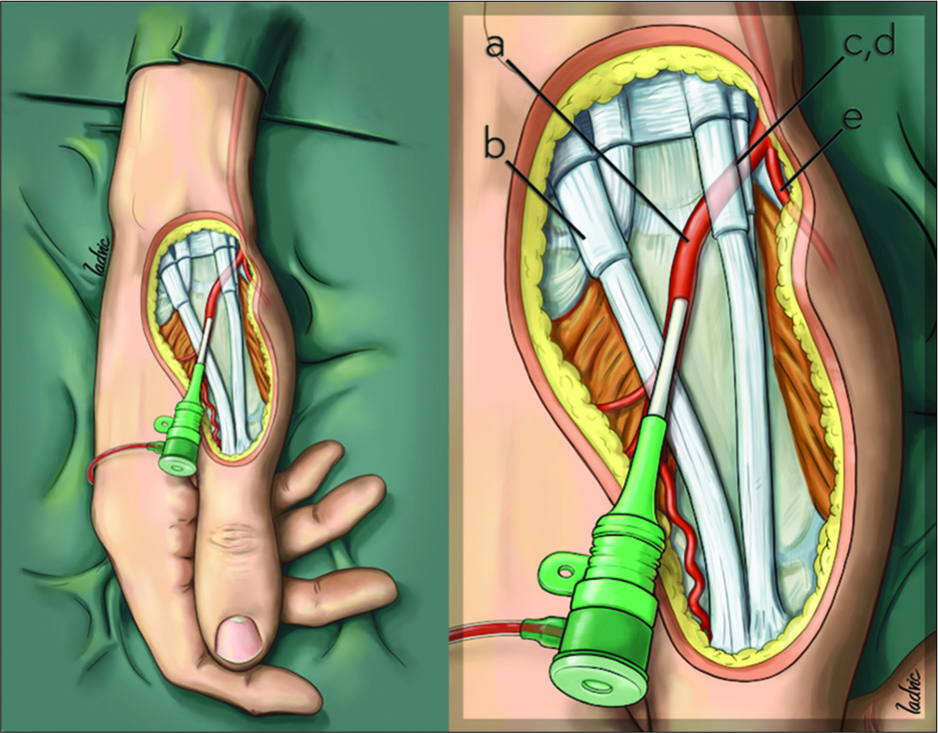
Figure 5:
Positioning of hand and anatomical landmarks for distal radial approach with the sheath located inside the radial artery. (a) Radial artery, (b) extensor pollicis longus tendon, (c) extensor pollicis brevis tendon, (d) abductor pollicis longus tendon, and (e) superficial palmar branch of the radial artery.
If the radial artery is not identified at the distal level, the hand is placed in supination and infiltration is performed approximately 2 cm above the wrist, where the radial pulse was marked in the pulse channel, according to a technique already described.[
In programmed therapeutic cases, where it is not necessary to perform a 4-vessel diagnostic procedure, navigation is initially performed with a Chaperon guide catheter mounted on a Simmons catheter (MicroVention Inc., Tustin, CA, USA), while directly conducting catheterization of the carrier vessel with the guide catheter. In the remaining patients, in whom treatment is performed using the same procedure after diagnosis completed with a Simmons Type II catheter (Merit Medical Systems, Utah, USA), a 260 cm-long hydrophilic guide wire is passed through the external carotid artery and replacement made on the corresponding external carotid artery utilizing either one of two guide catheters: Guider Softip XF 6F (Stryker, Neurovascular Fremont, CA, USA), Navien (Medtronic Neurovascular, Irvine, CA, USA), or Sophia (MicroVention Inc., Tustin, CA, USA). Once in the vessel with pathology, the procedure continues as with any approach [
In one patient in whom there was a vertebrovertebral aneurysm, whereby vertebrobasilar flow diversion and occlusion of the contralateral artery had to be performed, both a right radial and left distal radial approach were used, with entrance of the guiding catheters into both vertebral arteries [
Data analysis
Demographic and baseline clinical characteristics of the two patient cohorts – period 1 (last 3 months before distal radial approach use) and period 2 (first 3 months during which distal radial approach began to use) – were compared. Also were compared the rates at wich the femoral approach had to be used, overall and by gender.
RESULTS
Between March 25, 2019, and June 24, 2019 (period 2), a total of 94 endovascular procedures and 95 arterial punctures were performed (one procedure required a bilateral approach). Of these 94 procedures, 67 were diagnostic and 27 therapeutic; 27 (28%) were approached via femoral approach, 49 (51%) by radial route, and 19 (20%) by distal radial route. Of the 27 embolizations, 13 (48%) were performed through the radial approach, six (22%) through the femoral approach, and eight (30%) using the distal radial approach. Of the 68 punctures for angiography, 21 (30%) were performed through the femoral route, 36 (53%) by radial route, and 11 (16%) by distal radial route.
During period 1 (described previously), 80 procedures had been performed within the same two institutions: 65 diagnostic and 15 therapeutic, among which 38 had utilized the femoral route (47.5%) and 42 the radial route (52.5%). Of the 15 embolizations, two had been performed with radial approach and 13 through femoral approach. Of the angiographies, 40 (62%) and 25 (38%) had been done by radial and femoral route, respectively.
The mean age of patients in the first and second periods was 48 and 52 years old, respectively. The distribution by gender during the first period was 43 women and 37 men and in the second period 56 women and 38 men. In the first period, radial artery catheterization was used in 56% of the women, while in the second period when dTRA was added, the percentage of radial catheterization increased to 61% of the cases. In men, radial artery approach increased from 39% to 83%.
In this experience, using the dTRA as the first option for neuroendovascular procedures, 20% of the procedures were successful, with the full procedure completed through this approach. Of the therapeutic procedures (embolizations), 30% were successfully completed using the distal radial route, while success only was attained in 16% of the diagnostic procedures (cerebral angiographies).
When compared to a similar number of procedures performed over a similar period of time, we observed a reduction in the percentage of femoral approaches performed after adopting the dTRA as an option, from 47.5% to 28%. If only the embolizations are compared, we also observed a decline in the percentage of femoral approaches (from 87% to 22% of cases). If we compare the percentage of femoral approaches used for angiographies, the percentage fell from 38% to 30%. These data show an overall reduction in the rate of femoral approach use, both either for diagnostic or therapeutic purposes when the initial approach was distal radial. This trend did not change when men and women were analyzed separately.
Of the 27 embolizations performed within the second period, eight employed the distal radial approach, 13 the radial one, and only six the femoral route, meaning a significant decreased of femoral approaches.
The most obvious explanation for the observed decrease in femoral approaches between periods 1 and 2 is that when you start with a distal radial approach, you have a second option before resorting to the femoral route, which is not available if you begin with the classic radial approach. In this way, we can assume that at least some of the patients who ended up requiring a femoral procedure during the first period might have been spared that if the distal radial approach had been used initially.
CONCLUSION
Puncture of the radial artery within the anatomical snuffbox is another radial approach option for diagnostic and therapeutic neuroendovascular procedures and it appears to decrease the rate at which a femoral approach must ultimately be used.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Agostoni P, Biondi-Zoccai GG, de Benedictis ML, Rigattieri S, Turri M, Anselmi M. Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures; systematic overview and meta-analysis of randomized trials. J Am Coll Cardiol. 2004. 44: 349-56
2. Brunet MC, Chen SH, Sur S, McCarthy DJ, Snelling B, Yavagal DR. Distal transradial access in the anatomical snuffbox for diagnostic cerebral angiography. J Neurointerv Surg. 2019. 11: 710-3
3. Goland J, Doroszuk G. Transradial approach for endovascular diagnosis and treatment of ruptured cerebral aneurysms: A descriptive study. Surg Neurol Int. 2019. 10: 87-
4. Goland J, Doroszuk GF, Garbugino SL, Ypa MP. Transradial approach to treating endovascular cerebral aneurysms: Case series and technical note. Surg Neurol Int. 2017. 8: 73-
5. Jo KW, Park SM, Kim SD, Kim SR, Baik MW, Kim YW. Is transradial cerebral angiography feasible and safe? A single center’s experience. J Korean Neurosurg Soc. 2010. 47: 332-7
6. Kim JH, Park YS, Chung CG, Park KS, Chung DJ, Kim HJ. Feasibility and utility of transradial cerebral angiography: Experience during the learning period. Korean J Radiol. 2006. 7: 7-13
7. Ludman PF, Stephens NG, Harcombe A, Lowe MD, Shapiro LM, Schofield PM. Radial versus femoral approach for diagnostic coronary angiography in stable angina pectoris. Am J Cardiol. 1997. 79: 1239-41
8. Roh JH, Lee JH. Distal radial approach through the anatomical snuff box for coronary angiography and percutaneous coronary intervention. Korean Circ J. 2018. 48: 1131-4
9. Snelling BM, Sur S, Shah SS, Caplan J, Khandelwal P, Yavagal DR. Transradial approach for complex anterior and posterior circulation interventions: Technical nuances and feasibility of using current devices. Oper Neurosurg (Hagerstown). 2019. 17: 293-302
10. Snelling BM, Sur S, Shah SS, Khandelwal P, Caplan J, Haniff R. Transradial cerebral angiography: Techniques and outcomes. J Neurointerv Surg. 2018. 10: 874-81
11. Wretowski D, Krakowian M, Łabyk A, Pruszczyk P, Roik M. Very distal transradial approach (VITRO) for coronary interventions. Postepy Kardiol Interwencyjnej. 2019. 15: 42-5


Jim Ausman
Posted December 1, 2019, 7:38 am
Very nice approach to interventional diagnosis and treatments. What were the reasons you had to resort to the femoral approach in some patients? Any technical difficulties in reaching the cerebral vessels or using coils or stents? Do you see this approach becoming the route of choice?