

- Department of Neurosurgery, Kurume University School of Medicine, Fukuoka, Japan
- Department of Pathology, Kurume University School of Medicine, Fukuoka, Japan
Correspondence Address:
Motohiro Morioka
Department of Neurosurgery, Kurume University School of Medicine, Fukuoka, Japan
DOI:10.4103/2152-7806.170466
Copyright: © 2015 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yoshitomi M, Uchikado H, Hattori G, Sugita Y, Morioka M. Endoscopic biopsy for the diagnosis of neurosarcoidosis at the fourth ventricle outlet with hydrocephalus. Surg Neurol Int 25-Nov-2015;6:
How to cite this URL: Yoshitomi M, Uchikado H, Hattori G, Sugita Y, Morioka M. Endoscopic biopsy for the diagnosis of neurosarcoidosis at the fourth ventricle outlet with hydrocephalus. Surg Neurol Int 25-Nov-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/endoscopic-biopsy-for-the-diagnosis-of-neurosarcoidosis-at-the/
Abstract
Background:Fourth ventricle mass lesion in neurosarcoidosis is very rare and difficult to be diagnosed pathologically. We report a rare case of progressive hydrocephalus associated with neurosarcoidosis mass lesion located at the fourth ventricle outlet and suprasellar region.
Case Description:A 23-year-old man had a disturbance of consciousness and neck stiffness with fever. Magnetic resonance imaging revealed diffuse leptomeningeal enhancement, and the obstructive mass lesions at the outlet of the fourth ventricle. We performed an endoscopic biopsy of the enhanced lesion at the foramen Magendie, via foramen Monro and the aqueduct of the midbrain. Pathologically, the diagnosis of neurosarcoidosis was confirmed, and we started treatment with prednisolone. His neurological symptoms disappeared after ventriculo-peritoneal shunt and steroid therapy, and he was discharged without deficit 40 days after emergent admission.
Conclusion:Endoscopic procedure is less invasive and more effective for biopsy of neurosarcoidosis with hydrocephalus, even if the lesion is located at the fourth ventricle outlet.
Keywords: Endoscopic surgery, neurosarcoidosis, obstructive hydrocephalus
INTRODUCTION
Sarcoidosis is a chronic, multisystem, and granulomatous disorder of unknown etiology, which is most commonly recognized in young adults between the ages of 20 and 40 years. It commonly affects the lungs, eyes, lymph nodes, skin, and liver, but the involvement of the central nervous system is not common, ranging from 5% to 20%.[
In this case study, we report a rare case of rapid progressive hydrocephalus due to the obstruction of the fourth ventricle outlet that was pathologically diagnosed as fourth ventricle sarcoidosis by endoscopic biopsy.
CASE REPORT
A 23-year-old Japanese man was transferred to our hospital because of progressive consciousness disturbances with vomiting. He had no history of any systemic diseases but had a mild fever and headache frequently in 3 weeks prior to admission. He showed abnormal behavior from 14 days before hospitalization and eventually developed disturbance of consciousness. On admission, he showed nystagmus and neck stiffness with a fever of 38.5°C, and his Glasgow Coma Scale (GCS) score was 9 [E (3) V (1) M (5)]. Brain computed tomography (CT) revealed hydrocephalus with all ventricles dilated. We could not find any mass lesions on the CT-scan images. We performed external ventricular drainage (EVD) emergently, and his consciousness gradually improved. After emergent EVD, the magnetic resonance imaging (MRI) revealed diffuse leptomeningeal enhancement, and obvious enhanced mass lesion at the inferior wall of the third ventricle extended to the suprasellar region [Figure
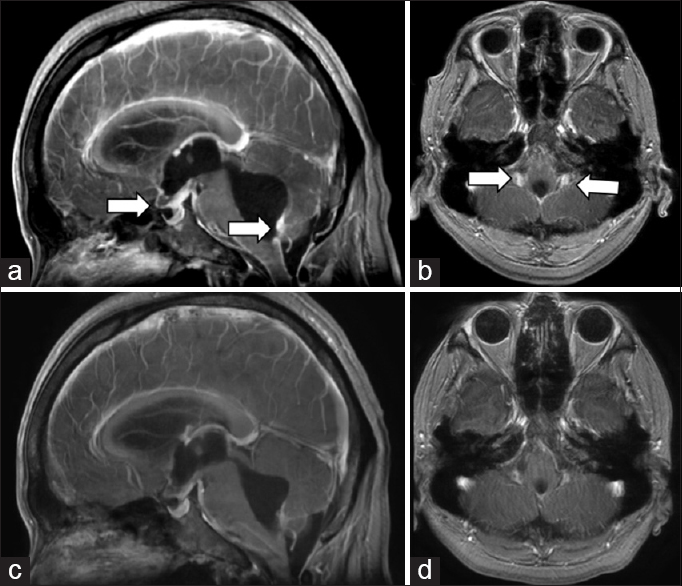
Figure 1
Radiological findings. (a and b) Initial magnetic resonance imaging study revealed leptomeningeal enhancement especially at the inferior portion of the fourth ventricle and suprasellar region (white arrows), ventricles were dilated. (c and d) In posterior fossa, bilateral mass located in the lower part of both foramina Luschka and midline mass located just superior from the foramen Magendie. Follow-up magnetic resonance imaging (1 week after steroid treatment) showed attenuation of the leptomeningeal enhanced lesions and hydrocephalus was improved
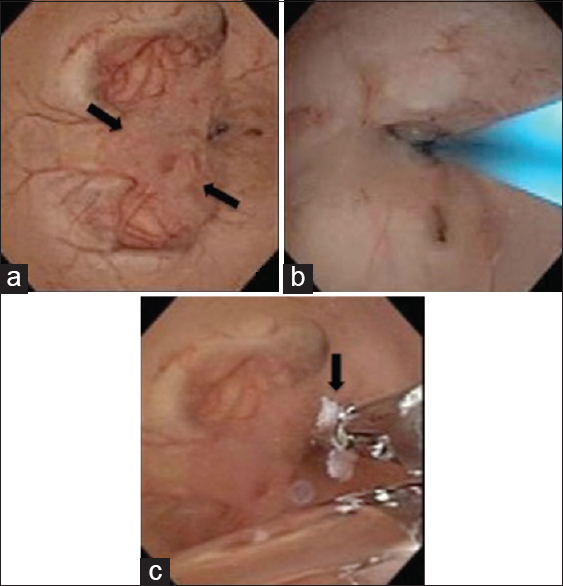
Figure 2
Intraoperative findings of the fourth ventricle floor. (a) the protruding mass lesions located just superior from the foramen Magendie (black arrows) and outlet of the fourth ventricle was obstructed by nodular lesions. (b) Ventriculostomy was performed at the obstruction of the fourth ventricle outlet. (c) Biopsy of the nodular lesions by endoscopy using forceps
DISCUSSION
Sarcoidosis is a multisystem, noncaseous granulomatous disease of unknown etiology. Neurological manifestation of sarcoidosis are observed in approximately 5–20% of patients with sarcoidosis.[
Here, we present a rare case of hydrocephalus with neurosarcoidosis. Our data suggests that endoscopic biopsy can enable “definite” diagnosis of neurosarcoidosis. We suggest that endoscopic surgery for hydrocephalus associated with neurosarcoidosis is not only therapeutic but also a biopsy tool for diagnosis. Endoscopic procedures are less invasive and effective for hydrocephalus associated with neurosarcoidosis, even when located at the floor of the foramen of fourth ventricle, and can be considered regularly in clinical practice.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We thank Ms. Keiko Suematsu for technical assistance. This work was supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Sports, Science, and Culture of Japan. We would like to thank Editage (www.editage.jp) for English language editing.
References
1. Akhondi H, Barochia S, Holmström B, Williams MJ. Hydrocephalus as a presenting manifestation of neurosarcoidosis. South Med J. 2003. 96: 403-6
2. Allen RK, Sellars RE, Sandstrom PA. A prospective study of 32 patients with neurosarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2003. 20: 118-25
3. Baussart B, Lepeintre JF, Tadié M. Endoscope-assisted biopsy for the diagnosis of neurosarcoidosis. Neurochirurgie. 2006. 52: 371-5
4. Dutra LA, Braga-Neto P, Oliveira RA, Pedroso JL, Abrahão A, Barsottini OG. Neurosarcoidosis: Guidance for the general neurologist. Arq Neuropsiquiatr. 2012. 70: 293-9
5. Hamada H, Hayashi N, Kurimoto M, Umemura K, Hirashima Y, Endo S. Isolated third and fourth ventricles associated with neurosarcoidosis successfully treated by neuroendoscopy – case report. Neurol Med Chir (Tokyo). 2004. 44: 435-7
6. Hesselmann V, Wedekind C, Terstegge K, Schulte O, Voges J, Krug B. An isolated fourth ventricle in neurosarcoidosis: MRI findings. Eur Radiol. 2002. 12: S1-3
7. Kim SH, Lee SW, Sung SK, Son DW. Treatment of hydrocephalus associated with neurosarcoidosis by multiple shunt placement. J Korean Neurosurg Soc. 2012. 52: 270-2
8. Lacomis D. Neurosarcoidosis. Curr Neuropharmacol. 2011. 9: 429-36
9. Miscusi M, Polli FM, Missori P, Delfini R. Ghost lesions in patient with cerebral-isolated neurosarcoidosis. A case report. J Neurosurg Sci. 2006. 50: 17-20
10. Naqi R, Azeemuddin M. Neurosarcoidosis. J Pak Med Assoc. 2012. 62: 293-4
11. Nozaki K, Scott TF, Sohn M, Judson MA. Isolated neurosarcoidosis: Case series in 2 sarcoidosis centers. Neurologist. 2012. 18: 373-7

