

- Department of Neurosurgery, Nara Medical University, Nara Prefecture, Japan
- Department of Radiology, Nara Medical University, Nara Prefecture, Japan
DOI:10.25259/SNI-94-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yudai Morisaki, Ichiro Nakagawa, Koji Omoto, Takeshi Wada, Kimihiko Kichikawa, Hiroyuki Nakase. Endovascular treatment of idiopathic intracranial hypertension caused by multiple venous sinus stenoses. 26-Mar-2019;10:47
How to cite this URL: Yudai Morisaki, Ichiro Nakagawa, Koji Omoto, Takeshi Wada, Kimihiko Kichikawa, Hiroyuki Nakase. Endovascular treatment of idiopathic intracranial hypertension caused by multiple venous sinus stenoses. 26-Mar-2019;10:47. Available from: http://surgicalneurologyint.com/surgicalint-articles/9237/
Date of Submission
14-Dec-2018
Date of Acceptance
02-Jan-2019
Date of Web Publication
26-Mar-2019
Abstract
Background: Idiopathic intracranial hypertension (IIH) shows symptoms by elevating intracranial pressure. Although sinus stenosis has been detected in many patients with IIH, the role of sinus stenosis in IIH remains obscure. Endovascular treatment for IIH due to transverse sinus stenosis has been frequently documented; however, IIH due to multiple sinus stenoses including the superior sagittal sinus (SSS) is rare. Here, we report a case of IIH due to multiple sinus stenoses treated by sinus stenting.
Case Presentation: A 47-year-old woman suffered from intractable headache with IIH presented with stenosis of the right transverse and SSS. Stent placement was carried out since intracranial hypertension and trans-stenotic cerebral venous pressure gradient (CVPG) were presented, and her intractable headache disappeared.
Conclusion: IIH can be caused by venous sinus stenoses and stent placement could be an appropriate treatment in patients who demonstrated a CVPG.
Keywords: Cerebral venous pressure gradient, idiopathic intracranial hypertension, sinus stenting, venous sinus stenosis
INTRODUCTION
Idiopathic intracranial hypertension (IIH) is a neurological failure caused by elevated intracranial pressure (ICP) in the absence of intracranial mass lesion.[
CASE PRESENTATION
A 47-year-old woman visited to our institute with a history of chronic intractable headache. Ophthalmologic evaluation demonstrated bilateral papilledema. We examined magnetic resonance (MR) venography depicted stenosis in the right transverse-sigmoid sinus and SSS stenosis [
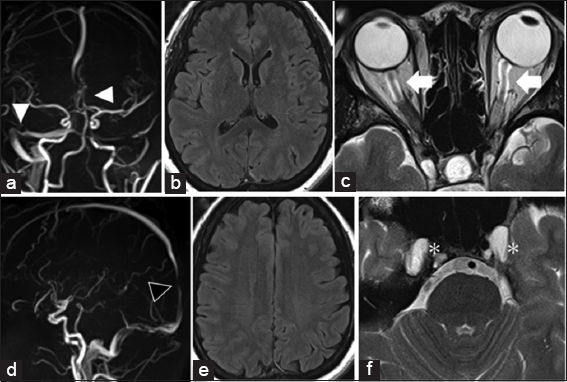
Figure 1
Magnetic resonance venography showed stenosis in the right transverse-sigmoid. (a) (White arrowheads) and in the superior sagittal sinus. (b) (Black arrowhead). On fluid-attenuated inversion recovery imaging, no ventricular enlargement or hydrocephalus is seen. (c and d). On T2-weighted imaging demonstrates accumulated cerebrospinal fluid in the bilateral optic nerve sheaths (white arrow). (e) And expansion of bilateral Meckel caves bilaterally (asterisk) (f).
Before endovascular treatment, the venous sinus pressure gradient was measured. The right internal carotid artery angiography revealed severe stenotic change in the right transverse-sigmoid sinus and SSS [
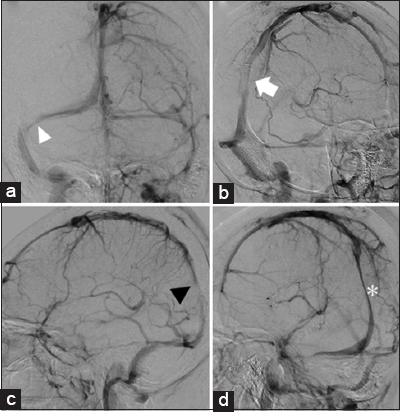
Figure 2
The left internal carotid artery angiography reveals severe stenosis in the right transverse-sigmoid sinus and superior sagittal sinus. (a) Anteroposterior view (white arrowhead). (b) Lateral view (black arrowhead). (c) Right anterior oblique view (white arrow), and. (d) Left anterior oblique view (asterisk).
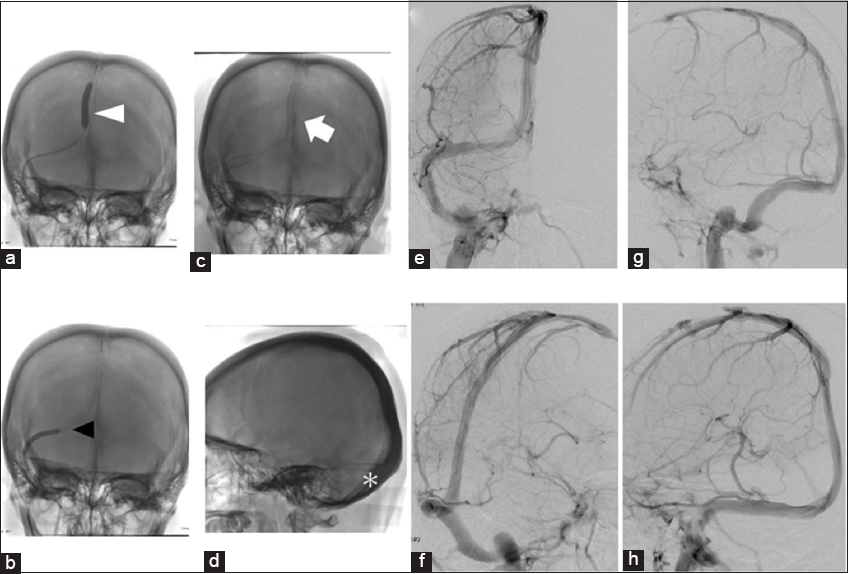
Figure 3
Percutaneous transluminal angioplasty was performed using a 4 mm × 40 mm Jackal in the superior sagittal sinus (SSS) (white arrowhead). (a) And transverse sinus (TS) (black arrowhead) (b). Stenting is performed in the SSS and right TS portion because each venous pressure gradient had not improved. (c) (White arrow). (d) (Asterisk). The right ICAG demonstrates satisfactory stent patency 3 months after the treatment. (e) Anteroposterior view. (f) Right anterior oblique view. (g) Lateral view; and. (h) Left anterior oblique view.
DISCUSSION
IIH often happens in young, obesity women who are between 20 and 50-year-old.[
TSS stenosis is found on MRV in most patients with IIH, with a specificity of 93% and a sensitivity of 93%.[
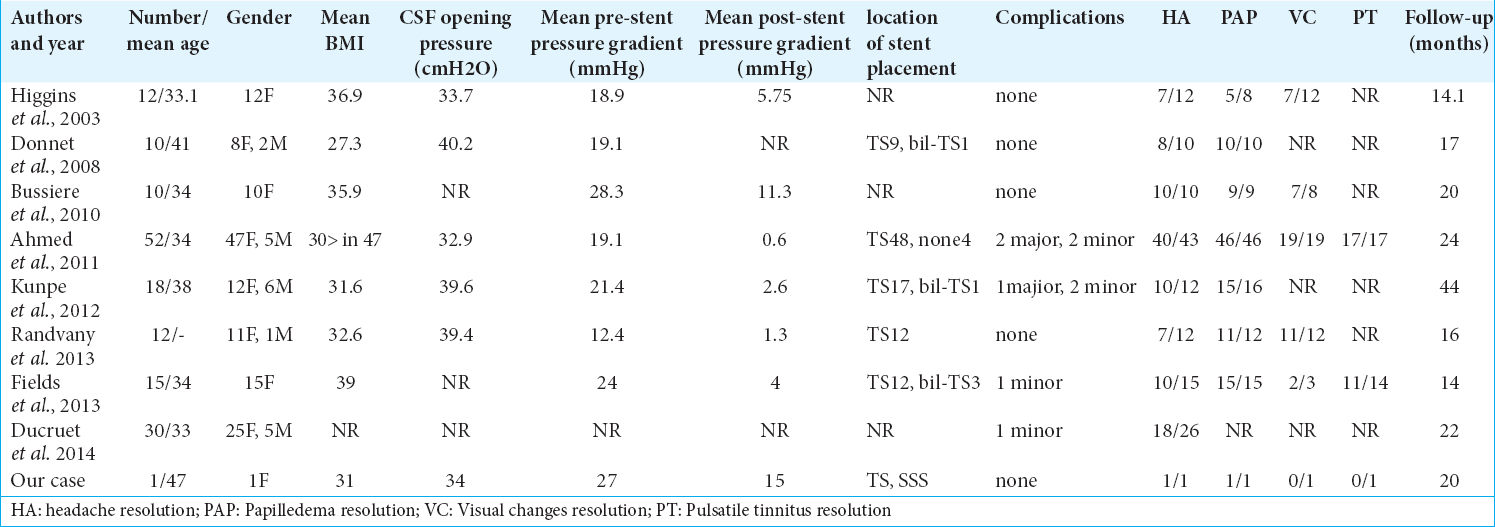
We found eight clinical reports in which intravascular therapy was used for venous sinus stenosis with CVPG [
Following MRI and MRV are important for an evaluation of instent restenosis after sinus stent placement because advent of instent restenosis has been recognized by some reports.[
CONCLUSION
Endovascular treatment of sinus stenoses is an attractive attention over the past 10 years. We should consider stent placement to treat in patients not responding to anticoagulant therapy or CSF shunting.
Compliance with ethical standards
The procedures performed were in accordance with the ethical standards of the Institutional Ethics Committee and with the 1975 Helsinki declaration and its later amendments.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ahmed RM, Wilkinson M, Parker GD, Thurtell MJ, Macdonald J, McCluskey PJ. Transverse sinus stenting for idiopathic intracranial hypertension: A review of 52 patients and of model predictions. AJNR Am J Neuroradiol. 2011. 32: 1408-14
2. Albuquerque FC, Dashti SR, Hu YC, Newman CB, Teleb M, McDougall CG. Intracranial venous sinus stenting for benign intracranial hypertension: Clinical indications, technique, and preliminary results. World Neurosurg. 2011. 75: 648-52
3. Arac A, Lee M, Steinberg GK, Marcellus M, Marks MP. Efficacy of endovascular stenting in dural venous sinus stenosis for the treatment of idiopathic intracranial hypertension. Neurosurg Focus. 2009. 27: E14-
4. Bussière M, Falero R, Nicolle D, Proulx A, Patel V, Pelz D. Unilateral transverse sinus stenting of patients with idiopathic intracranial hypertension. AJNR Am J Neuroradiol. 2010. 31: 645-50
5. De Simone R, Ranieri A, Bonavita V. Advancement in idiopathic intracranial hypertension pathogenesis: Focus on sinus venous stenosis. Neurol Sci. 2010. 31: S33-9
6. Donnet A, Metellus P, Levrier O, Mekkaoui C, Fuentes S, Dufour H. Endovascular treatment of idiopathic intracranial hypertension: Clinical and radiologic outcome of 10 consecutive patients. Neurology. 2008. 70: 641-7
7. Ducruet AF, Crowley RW, McDougall CG, Albuquerque FC. Long-term patency of venous sinus stents for idiopathic intracranial hypertension. J Neurointerv Surg. 2014. 6: 238-42
8. Fields JD, Javedani PP, Falardeau J, Nesbit GM, Dogan A, Helseth EK. Dural venous sinus angioplasty and stenting for the treatment of idiopathic intracranial hypertension. J Neurointerv Surg. 2013. 5: 62-8
9. Higgins JN, Cousins C, Owler BK, Sarkies N, Pickard JD. Idiopathic intracranial hypertension: 12 cases treated by venous sinus stenting. J Neurol Neurosurg Psychiatry. 2003. 74: 1662-6
10. Kumpe DA, Bennett JL, Seinfeld J, Pelak VS, Chawla A, Tierney M. Dural sinus stent placement for idiopathic intracranial hypertension. J Neurosurg. 2012. 116: 538-48
11. Levitt MR, Hlubek RJ, Moon K, Kalani MY, Nakaji P, Smith KA. Incidence and predictors of dural venous sinus pressure gradient in idiopathic intracranial hypertension and non-idiopathic intracranial hypertension headache patients: Results from 164 cerebral venograms. J Neurosurg. 2017. 126: 347-53
12. Radvany MG, Solomon D, Nijjar S, Subramanian PS, Miller NR, Rigamonti D. Visual and neurological outcomes following endovascular stenting for pseudotumor cerebri associated with transverse sinus stenosis. J Neuroophthalmol. 2013. 33: 117-22
13. Smith KA, Peterson JC, Arnold PM, Camarata PJ, Whittaker TJ, Abraham MG. Acase series of dural venous sinus stenting in idiopathic intracranial hypertension: Association of outcomes with optical coherence tomography. Int J Neurosci. 2017. 127: 145-53
14. Yamaguchi R, Sato K, Fujimaki K, Takakura K. A case of stent placement for intracranial hypertension associated with venous sinus stenosis. J Neuroendovascular Ther. 2017. 11: 203-8

