

- Departments of Neurosurgery, Nara Hospital, Kindai University, Ikoma, Nara, Japan,
- Departments of Neurosurgery, Yuaikai Hospital, Suminoe-ku, Osaka, Osaka-fu, Japan.
Correspondence Address:
Akira Watanabe
Departments of Neurosurgery, Nara Hospital, Kindai University, Ikoma, Nara, Japan,
DOI:10.25259/SNI-246-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Akira Watanabe, Kinya Nakanishi, Kazuo Kataoka. Intradural spinal arachnoid cyst contributing to sudden paraparesis. 19-Jun-2019;10:102
How to cite this URL: Akira Watanabe, Kinya Nakanishi, Kazuo Kataoka. Intradural spinal arachnoid cyst contributing to sudden paraparesis. 19-Jun-2019;10:102. Available from: http://surgicalneurologyint.com/surgicalint-articles/9382/
Date of Submission
12-Apr-2019
Date of Acceptance
02-May-2019
Date of Web Publication
19-Jun-2019
Abstract
Background: Spinal arachnoid cysts are cystic lesions filled with cerebrospinal fluid that contributes to neurological deficits depending on their size/location within the spinal canal. Here, we report a patient with a spinal subarachnoid cyst who suddenly developed paraparesis.
Case Description: A 37-year-old female with a thoracic spinal arachnoid cyst at the T7 level suddenly developed lower abdominal pain followed by immediate paraparesis. Two weeks following the onset of symptoms, she underwent a T6-T8 laminectomy; this included with full cyst excision. By the 4th postoperative week, her signs/symptoms fully resolved.
Conclusions: A 37-year-old female with a T7 thoracic spinal subarachnoid cyst who presented with acute paraparesis regained normal function 2 weeks following a T6-T8 laminectomy.
Keywords: Paraparesis, Spinal arachnoid cyst, Sudden onset, Valsalva-like maneuver
INTRODUCTION
Spinal arachnoid cysts are filled with cerebrospinal fluid (CSF). They may be congenital or acquired (e.g., occur after trauma, hemorrhage, infection, or iatrogenic insults). They can be extra- and intra-axial or intramedullary lesions and are maybe communicating or noncommunicating with the CSF space. Symptoms of spinal compression are rare but may include pain, hypesthesia, paresis, and sphincter dysfunction.[
CASE REPORT
A 37-year-old female presented with the sudden onset of abdominal pain rapidly accompanied by numbness and weakness in both lower extremities. On examination, she was paraparetic (right 3/5 and left 4/5 proximally/distally) and exhibited decreased pin, temperature, vibration, and position perception below the T8 level.
Diagnostic studies
The thoracic magnetic resonance image (MRI) revealed a dorsal intradural extramedullary cyst at the T7 level, compressing, and displacing the cord anteriorly. The T2-weighted image is showed a high-intensity uniform cyst (filled with cerebral spinal) [

Figure 1
Initial thoracic magnetic resonance image (T2-WI) (a) Sagittal view – an intradural extramedullary cyst was located at the T7 level dorsal to the spinal cord. (b) Axial view, serial cross-section around T7 – the cyst compressed the spinal cord anteriorly. The high intensity of the cyst on T2-WI is consistent with a cerebrospinal fluid filling.
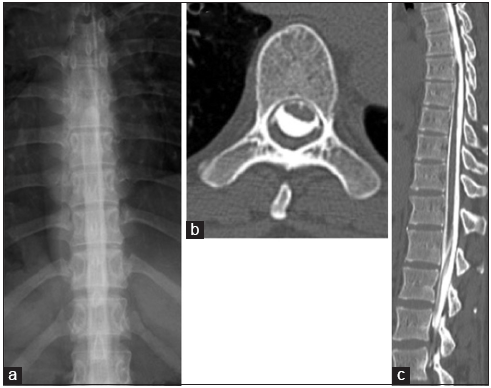
Figure 2
(a) Thoracic myelography (A-P image) – the contrast medium was blocked at the T7 level. (b) Thoracic axial computed tomography after myelography at the T7 level – the cyst was filled with contrast medium. (c) Thoracic sagittal computed tomography after myelography – the contrast medium filled both the subarachnoid space and the cyst uniformly.
Hospital course
Initially, the patient was treated conservatively with steroid therapy; indeed, she exhibited some gradual spontaneous improvement (e.g., able to walk without any support within 1 day). However, her ataxia and proprioceptive deficits in both legs persisted, and the spinal arachnoid cyst did not regress on the follow-up MRI. Surgery consisting of a T6-T8 hemilaminectomy, therefore, was performed 2 weeks after the onset of symptoms. Upon opening the dura mater, we found an arachnoid cyst with a thick whitened wall compressing the spinal cord. Notably, the cyst pulsated with each heartbeat and contained clear CSF fluid. There was, however, no documented communication between the cyst and the subarachnoid space. After removing the cyst, the histological examination confirmed the diagnosis of an arachnoid cyst. Two weeks postoperatively, the patient fully recovered.
DISCUSSION
Spinal arachnoid cysts are rarely symptomatic but occasionally contribute to slowly or occasionally rapidly progressive motor/sensory paraparesis and sphincter disturbance.[
Compression by enlarging cysts may contribute to spinal cord dysfunction. The mechanism of growth is typically due to fluid secretion from the cyst wall cell themselves, active transport of water according to osmotic gradient, or a one-way valve allowing fluid movement to the cyst after CSF pressure fluctuations.[
Valsalva-like maneuvers during daily activities, such as coughing, straining, standing up, and compressing the abdomen, can make large CSF pressure fluctuation due to distension of the epidural vein influenced by abdominal or thoracic cavity pressure changes.[
All instances of intradural extramedullary cysts, including our case, undergoing decompression/cyst removal, resulted in complete recovery.[
CONCLUSIONS
A 37-year-old female with a symptomatic intradural spinal arachnoid cyst at the T7 level presented with the sudden onset of paraparesis. The patient underwent a T6-T8 laminectomy 2 weeks after presentation, and she was asymptomatic by the 4th postoperative week.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Basaldella L, Orvieto E, Dei Tos AP, Della Barbera M, Valente M, Longatti P. Causes of arachnoid cyst development and expansion. Neurosurg Focus. 2007. 22: E4-
2. Bassiouni H, Hunold A, Asgari S, Hübschen U, König HJ, Stolke D. Spinal intradural juxtamedullary cysts in the adult: Surgical management and outcome. Neurosurgery. 2004. 55: 1352-9
3. Kerr JM, Ukpeh H, Steinbok P. Spinal extradural arachnoid cyst presenting as recurrent abdominal pain. Childs Nerv Sys. 2015. 31: 965-9
4. Lee HJ, Cho DY. Symptomatic spinal intradural arachnoid cysts in the pediatric age group: Description of three new cases and review of the literature. Pediatr Neurosurg. 2001. 35: 181-7
5. Maiuri F, Iaconetta G, Esposito M. Neurological picture. Recurrent episodes of sudden tetraplegia caused by an anterior cervical arachnoid cyst. J Neurol Neurosurg Psychiatry. 2006. 77: 1185-6
6. Petridis AK, Doukas A, Barth H, Mehdorn HM. Spinal cord compression caused by idiopathic intradural arachnoid cysts of the spine: Review of the literature and illustrated case. Eur Spine J. 2010. 19: S124-9
7. Wang MY, Levi AD, Green BA. Intradural spinal arachnoid cysts in adults. Surg Neurol. 2003. 60: 49-55

