

- Division of Neurosurgery, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
- Department of Pathology and Laboratory Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
- Department of Nursing, Meiho University, Taiwan
Correspondence Address:
Ying Tso Chen
Division of Neurosurgery, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
DOI:10.4103/sni.sni_467_17
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Chi-Man Yip, Huai-Pao Lee, Shu-Shong Hsu, Ying Tso Chen. Left orbital roof giant cell tumor of bone: A case report. 26-Jun-2018;9:127
How to cite this URL: Chi-Man Yip, Huai-Pao Lee, Shu-Shong Hsu, Ying Tso Chen. Left orbital roof giant cell tumor of bone: A case report. 26-Jun-2018;9:127. Available from: http://surgicalneurologyint.com/surgicalint-articles/left-orbital-roof-giant-cell-tumor-of-bone-a-case-report/
Date of Submission
06-Dec-2017
Date of Acceptance
23-May-2018
Date of Web Publication
26-Jun-2018
Abstract
Background:Giant cell tumor of bone originating from the connective tissue within the bone marrow is benign but locally aggressive lesion. In all, 90% of the cases involve the epiphysis of long bones and less than 2% involve the skull. Giant cell tumors of the skull occur most frequently in the sphenoid and temporal bones, and very rarely in the ethmoid, frontal, parietal, and occipital bones. We would like to share a case of giant cell tumor of bone arising from the left orbital roof with involving ethmoid sinus, which was diagnosed to be a meningioma before surgery.
Case Description:A 32-year-old lady presented to us with the chief complain of left proptosis, diplopia, and left eye soreness without decline of visual acuity for about 2 months. Her orbital magnetic resonance imaging (MRI) disclosed a mass lesion located in the left frontal base, orbital roof, and upper medial orbital region with adjacent dural-tail sign favoring meningioma. She underwent a left supraorbital pterional craniotomy with the gross total removal of tumor and dura reconstruction. Histology examination of the tumor showed a picture of giant cell tumor of bone. Considering giant cell tumor of bone is locally aggressive, postoperative adjuvant therapy with Denosumab was introduced after full explanation.
Conclusion:Standard treatments of skull-base giant cell tumors have yet to be established due to small number of cases reported in the literature. The standard treatment of giant cell tumor of bone is complete resection of the tumor.
Keywords: Anti-RANKL monoclonal antibody, giant cell tumor of bone, orbital roof tumor
INTRODUCTION
Giant cell tumor of bone was described by Cooper and Travers in 1818, which is characterized histologically by multinucleated giant cells with a background of mononuclear stromal cells.[
CASE REPORT
In March 2017, a 32-year-old woman without any systemic disease or ocular traumatic event presented to us with the chief complain of left proptosis, left eye soreness, and diplopia on upper right gaze without decline of visual acuity since January 2017. Noncontrast computed tomography (CT) of orbit done at an outside hospital showed a left intra-orbital tumor with intracranial invasion. Orbital magnetic resonance imaging (MRI) was arranged and it disclosed a mass lesion about 3.8 cm × 3.7 cm × 3.3 cm in size, located in the left frontal base, orbital roof, and upper medial orbital region. This mass lesion showed relative intermediate intensity on T1-weighted image and T2-weighted image, and the postcontrast study showed good enhancement with adjacent dural tail sign causing mass effect on the left eyeball as well as the left frontal brain parenchyma, which favored meningioma [
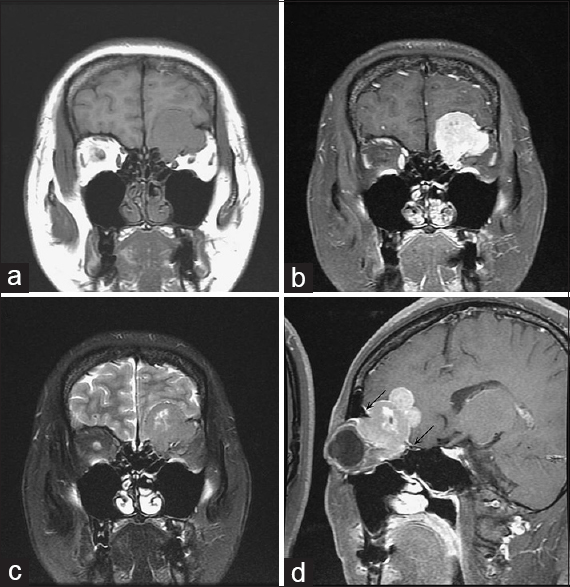
Figure 1
Preoperative orbit MRI. Coronal T1 weighted image (a), coronal T1 weighted image post gadolinium enhancement (b), coronal T2 weighted image (c), and sagittal T1 weighted image post gadolinium enhancement (d) showing a well-circumscribed lesion isointensity on T1-weighted images and hypointensity on T2-weighted image with good enhancement and has small cystic/necrotic change noted in the left frontal base, orbital roof, and upper-medial orbital region. The black arrows point out the dural tail sign
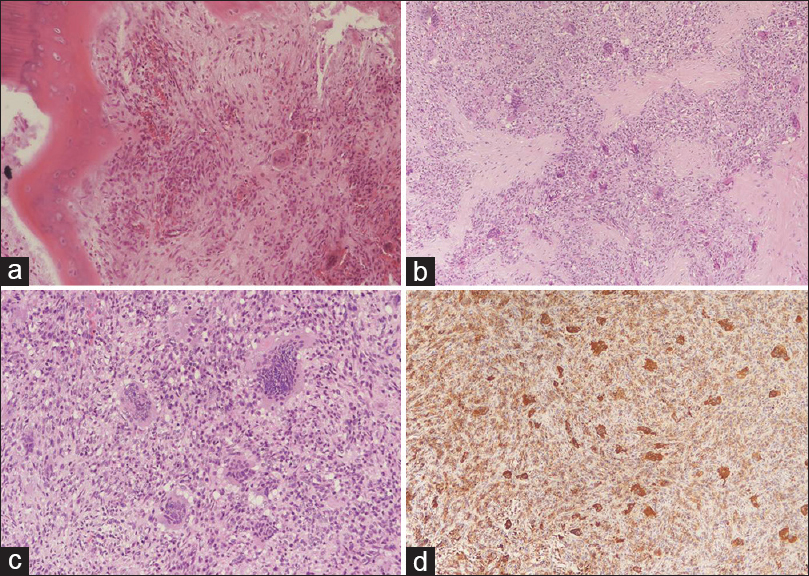
Figure 2
Histology of the specimen. Orbital roof HE stain 200X (a), Dura HE stain 100X (b), Tumor HE stain 200X (c) showing osteoclast-like giant cells in a background of round or spindle-shaped mononuclear cells. The resected orbital roof and dura had been involved by the tumor. Tumor CD68 stain 100X (d) showing positive staining. CD68 is particularly useful as a marker for giant cells, osteoclasts
DISCUSSION
Giant cell tumor of bone is an aggressive, bone lytic, osteoclastogenic stromal tumor.[
CONCLUSION
Orbitofrontal giant cell tumor of bone is very rare. To our best knowledge, only three cases had been reported in the English literature [

Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bardakhchyan S, Kager L, Danielyan S, Avagyan A, Karamyan N, Vardevanyan H. Denosumab treatment for progressive skull base giant cell tumor of bone in a 14 year old female- a case report and literature review. Ital J Pediatr. 2017. 43: 32-
2. Borkowska A, Goryn T, Pienkowski A, Wagrodzki M, Jagiello-Wieczorek E, Rogala P. Denosumab treatment of inoperable or locally advanced giant cell tumor of bone. Oncol Lett. 2016. 12: 4312-8
3. Chakarun CF, Forrester DM, Gottsegen CF, Patel DB, White EA, Matcuk GR. Giant Cell Tumor of Bone: Review, Mimics, and New Developments in Treatment. Radiographics. 2013. 33: 197-211
4. Cooper AS, Travers B.editors. Surgical essays. London, England: Cox Longman and Co; 1818. p. 178-9
5. Gaston CL, Grimer RJ, Parry M, Stacchiotti S, Tos APD, Gelderblom H. Current status and unanswered questions on the use of Denosumab in giant cell tumor of bone. Clin Sarcoma Res. 2016. 6: 15-
6. Goto Y, Furuno Y, Kawabe T, Ohwada K, Tatsuzawa K, Sasajima H. Treatment of a skull-base giant cell tumor with endoscopic endonasal resection and denosumab: Case report. J Neurosurg. 2017. 126: 431-4
7. Harris AE, Beckner ME, Barnes L, Kassam A, Horowitz M. Giant cell tumor of the skull: A case report and review of the literature. Surg Neurol. 2004. 61: 274-7
8. Kamoshima Y, Sawamura Y, Imai T, Furukawa H, Kubota K, Houkin K. Giant Cell Tumor of the Frontal Bone in a Girl- Case Report. Neurol Med Chir (Tokyo). 2011. 51: 798-800
9. Tang PH, Mettu P, Maltry AC, Harrison AR, Mokhtarzadeh A. Giant Cell Tumor of the Frontal Bone Presenting as an Orbital Mass. Ophthalmol Ther. 2017. 6: 215-20
10. Van der Heijden L, Dijkstra S, Blay JY, Gelderblom H. Giant cell tumour of bone in the denosumab era. Eur J Cancer. 2017. 77: 75-83
11. Van der Heijden L, Dijkstra S, Van de Sande MAJ, Kroep JR, Nout RA, Van Rijswijk CSP. The Clinical Approach Toward Giant Cell Tumor of Bone. Oncologist. 2014. 19: 550-61
12. Vernet O, Ducrey N, Deruaz JP, Tribolet ND. Giant Cell Tumor of the Orbit. Neurosurgery. 1993. 32: 848-51

