

- Professor of Clinical Neurosurgery, School of Medicine, University of State of New York at Stony Brook, Mineola, New York, USA
- Chief of Neurosurgical Spine/Education, NYU Winthrop Hospital, Mineola, New York, USA
Correspondence Address:
Nancy E. Epstein
Professor of Clinical Neurosurgery, School of Medicine, University of State of New York at Stony Brook, Mineola, New York, USA
Chief of Neurosurgical Spine/Education, NYU Winthrop Hospital, Mineola, New York, USA
DOI:10.4103/sni.sni_26_18
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nancy E. Epstein. Lower complication and reoperation rates for laminectomy rather than MI TLIF/other fusions for degenerative lumbar disease/spondylolisthesis: A review. 07-Mar-2018;9:55
How to cite this URL: Nancy E. Epstein. Lower complication and reoperation rates for laminectomy rather than MI TLIF/other fusions for degenerative lumbar disease/spondylolisthesis: A review. 07-Mar-2018;9:55. Available from: http://surgicalneurologyint.com/surgicalint-articles/lower-complication-and-reoperation-rates-for-laminectomy-rather-than-mi-tlif-other-fusions-for-degenerative-lumbar-disease-spondylolisthesis-a-review/
Date of Submission
22-Jan-2018
Date of Acceptance
25-Jan-2018
Date of Web Publication
07-Mar-2018
Abstract
Background:Utilizing the spine literature, we compared the complication and reoperation rates for laminectomy alone vs. instrumented fusions including minimally invasive (MI) transforaminal lumbar interbody fusion (TLIF) for the surgical management of multilevel degenerative lumbar disease with/without degenerative spondylolisthesis (DS).
Methods:Epstein compared complication and reoperation rates over 2 years for 137 patients undergoing laminectomy alone undergoing 2-3 level (58 patients) and 4-6 level (79 patients) Procedures for lumbar stenosis with/without DS. Results showed no new postoperative neurological deficits, no infections, no surgery for adjacent segment disease (ASD), 4 patients (2.9%) who developed intraoperative cerebrospinal fluid (CSF) fistulas, no readmissions, and just 1 reopereation for a (postoperative day 7). These rates were compared to other literature for lumbar laminectomies vs. fusions (e.g. particularly MI TLIF) addressing pathology comparable to that listed above.
Results:Some studies in the literature revealed an average 4.8% complication rate for laminectomy alone vs. 8.3% for decompressions/fusion; at 5 postoperative years, reoperation rates were 10.6% vs. 18.4%, respectively. Specifically, the MI TLIF literature complication rates ranged from 7.7% to 23.0% and included up to an 8.3% incidence of wound infections, 6.1% durotomies, 9.7% permanent neurological deficits, and 20.2% incidence of new sensory deficits. Reoperation rates (1.6–6%) for MI TLIF addressed instrumentation failure (2.3%), cage migration (1.26–2.4%), cage extrusions (0.8%), and misplaced screws (1.6%). The learning curve (e.g. number of cases required by a surgeon to become proficient) for MI TLIF was the first 33-44 cases. Furthermore, hospital costs for lumbar fusions were 2.6 fold greater than those for laminectomy alone, with overall neurosurgeon reimbursement quoted in one study as high as $142,075 per year.
Conclusions:The spinal literature revealed lower complication and reoperation rates for lumbar laminectomy alone vs. higher rates for instrumented fusion, including MI TLIF, for degenerative lumbar disease with/without DS.
Keywords: Complication rates, fusions, laminectomy alone, minimally invasive, reoperation rates, transforaminal lumbar interbody fusion
INTRODUCTION
When reviewing the literature, we asked whether lower complication and reoperation rates would be associated with performing multilevel laminectomy alone vs. fusions [e.g., predominantly minimally invasive (MI) transforaminal lumbar interbody fusion (TLIF)] for degenerative lumbar disease with/without degenerative spondylolisthesis (DS) [Tables
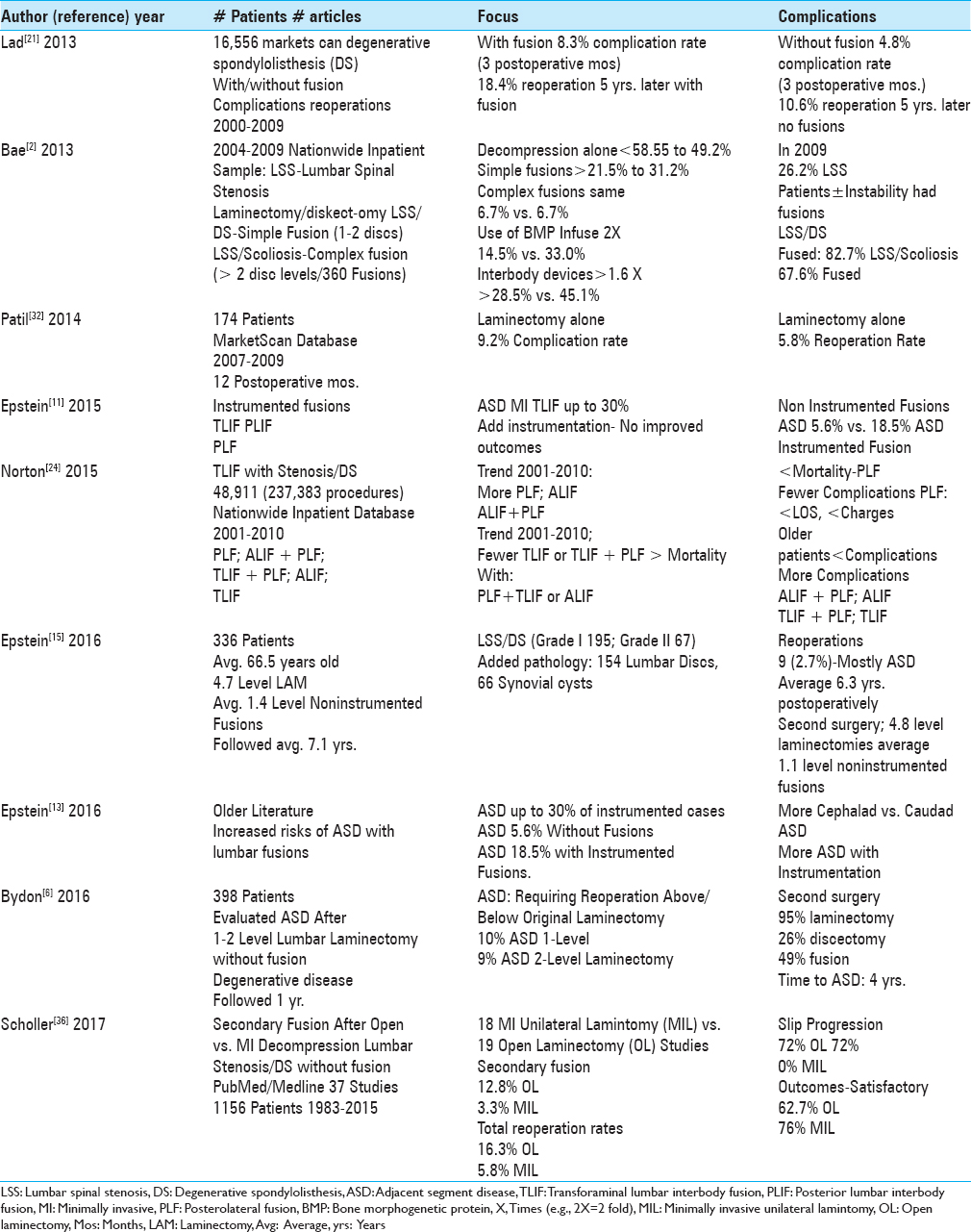
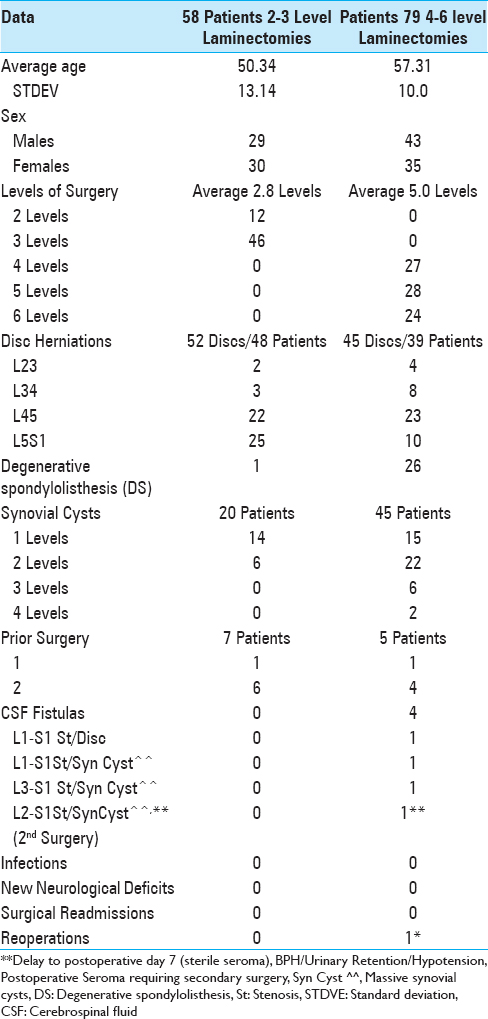
Table 2
Epstein series clinical data following 2-3 (58 patients) vs. 4-6 level (79 patients) lumbar laminectomies without fusions[
Trends toward more laminectomies/fusions vs. laminectomies alone for degenerative lumbar disease with/without degenerative spondylolisthesis (DS)
For lumbar degenerative disease with/without DS, several studies documented the increasing trend toward utilizing not only laminectomy for decompression but also adding instrumented fusions [
Complication and reoperation rates For laminectomy vs. fusions for degenerative lumbar disease with or without degenerative spondylolisthesis (DS)
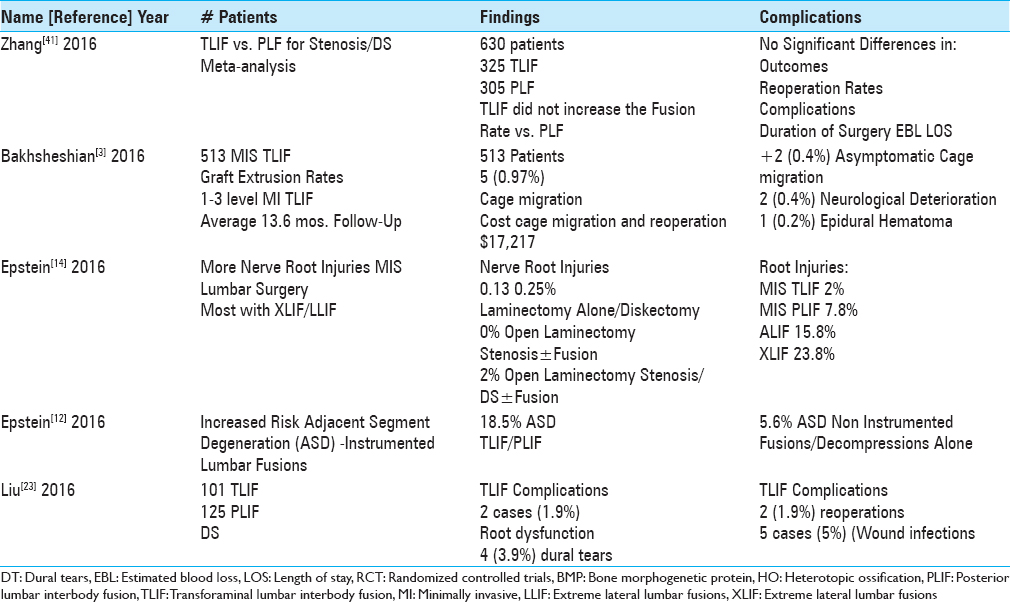
The surgical literature showed lower complication and/or reoperation rates utilizing decompressions alone vs. decompressions and fusions for degenerative lumbar disease with/without DS [
Less adjacent segment disease (ASD) for decompressions/noninstrumented fusions vs. instrumented fusions for degenerative lumbar disease/degenerative spondylolisthesis (DS)
Several articles documented a lower incidence of ASD following laminectomy/laminectomy with noninstrumented fusion vs. decompressions with instrumented lumbar fusions (ASD) [
Separate Epstein series showed reduced complication/reoperation rates with laminectomy alone without noninstrumented fusion for treating degenerative lumbar disease/degenerative spondylolisthesis (DS)
Epstein performed a prospective, consecutive cohort study regarding the efficacy of laminectomy alone for 137 patients with degenerative lumbar disease/with or without DS.[
Complication rate of minimally invasive transforaminal lumbar interbody fusion (MI TLIF) for degenerative lumbar disease without degenerative spondylolisthesis (DS)
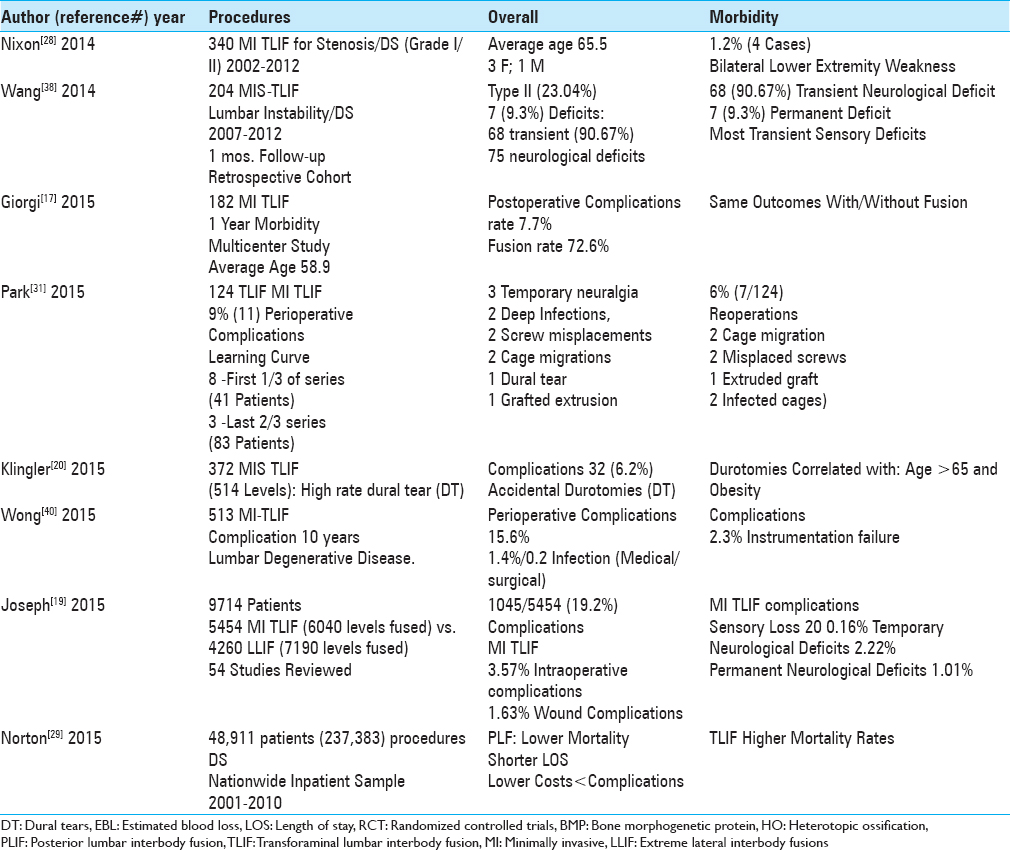
The overall complication rate for MI TLIF fusions addressing degenerative lumbar disease without DS ranged from 7.7% to 19.2% [Tables
Complication rate for minimally invasive transforaminal interbody lumbar fusion (MI TLIF) For degenerative lumbar disease with degenerative spondylolisthesis (DS)
The overall complication rate for MI TLIF addressing degenerative lumbar disease with DS ranged from 13% to 23.04% [Tables
Minimally invasive transforminal interbody lumbar fusion (MI TLIF)-related new postoperative neurological deficits
Permanent neurological deficits following MI TLIF occurred in 0.2–9.7% of patients [Tables
Frequency of dural tears with minimally invasive transforminal interbody lumbar fusion
Dural tears occurred in 3.9–6.1% of the patients undergoing MI-TLIF [Tables
Reoperation rates for minimally invasive transforminal interbody lumbar fusion (MI TLIF)
Reoperations, performed in between 1.6% of the patients following MI TLIF, were largely attributed to instrumentation failures [Tables
Up to 8.3% infection rates for minimally invasive transforaminal interbody lumbar fusion (MI TLIF)
Spinal infections occurred in from 0.2% up to 8.3% of patients undergoing predominantly MI TLIF [Tables
Mortality rates reported higher for transforminal interbody lumbar fusion (TLIF) vs. posterolateral lumbar fusion (PLF)
When Norton et al. (2015) reviewed 48,911 patients (237,383 procedures) from the Nationwide Inpatient Sample Database (2001 to 2010) with degenerative lumbar disease/DS, those undergoing TLIF had higher morality rates vs. those having posterolateral lumbar fusions (PLF). Indeed, performance of PLF correlated with lower mortality rates, reduced hospital charges, LOS, and complication rates) [
Restricted field of vision for minimally invasive transforaminal interbody lumbar fusion (MI TLIF)
Although Saetia et al. (2013) found similar complication rates of 8.3% for both open TLIF vs. MI TLIF for lumbar degenerative spondylolisthesis, the authors noted shortcomings of MI TLIF, including a restricted filed of vision (e.g. more limited exposure) that “required a very thorough knowledge of anatomy” [
Comparable outcomes for minimally invasive transforaminal lumbar fusion (MI TLIF) vs. other instrumented fusions including posterolateral lumbar fusion (PLF)
Multiple studies documented similar outcomes for MI TLIF/TLIF vs. other types of instrumented lumbar fusions (e.g., particularly PLF) [Tables
BMP/INFUSE (Medtronic, Memphis, TN, USA) increased risks and complications for lumbar fusions including posterior lumbar interbody fusion (PLIF)/transforaminal interbody fusion/minimally invasive transforaminal interbody fusion (TLIF/MI TLIF)
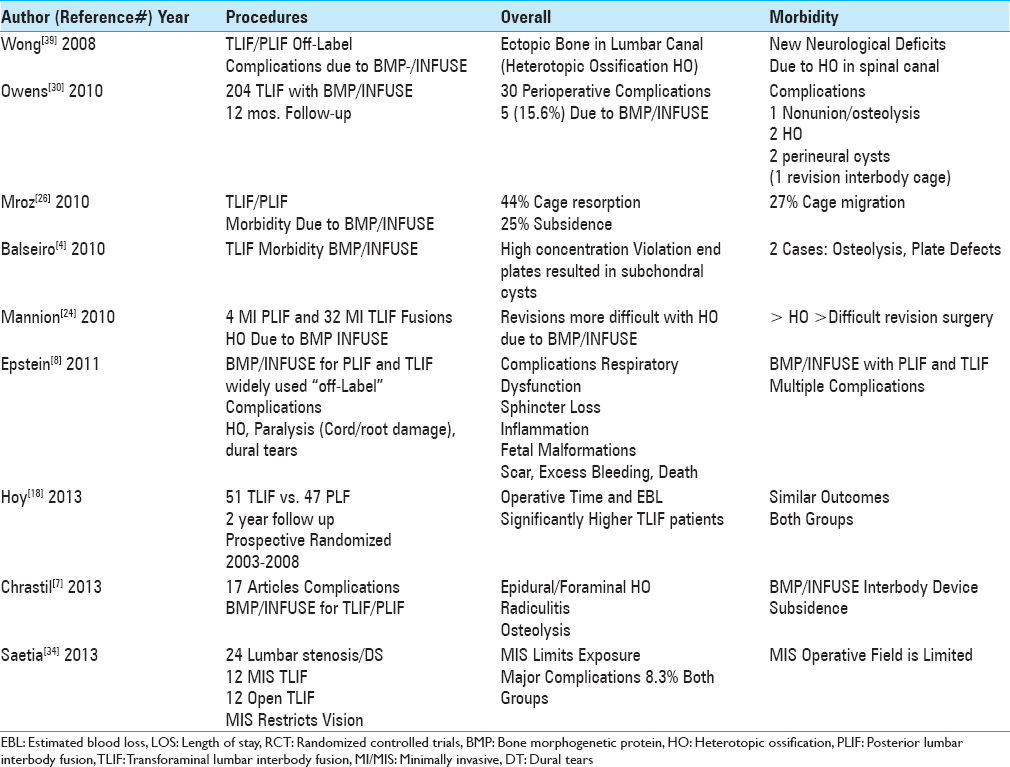
BMP (bone morphogenetic protein)/INFUSE (Medtronic, Memphis, TN, USA) was and is still frequently applied “off-label” (e.g. posteriorly in the lumbar spine) for performing posterior lumbar spinal fusions including PLIF/TLIF/MI TLIF, thus increasing the risks and complication rates [Tables
Obviously, the use of BMP/INFUSE for TLIF/MI TLIF, PLIF and other instrumented fusions introduces additional complications not seen with the laminectomy alone/laminectomy with non instrumented fusion where BMP is not utilized.
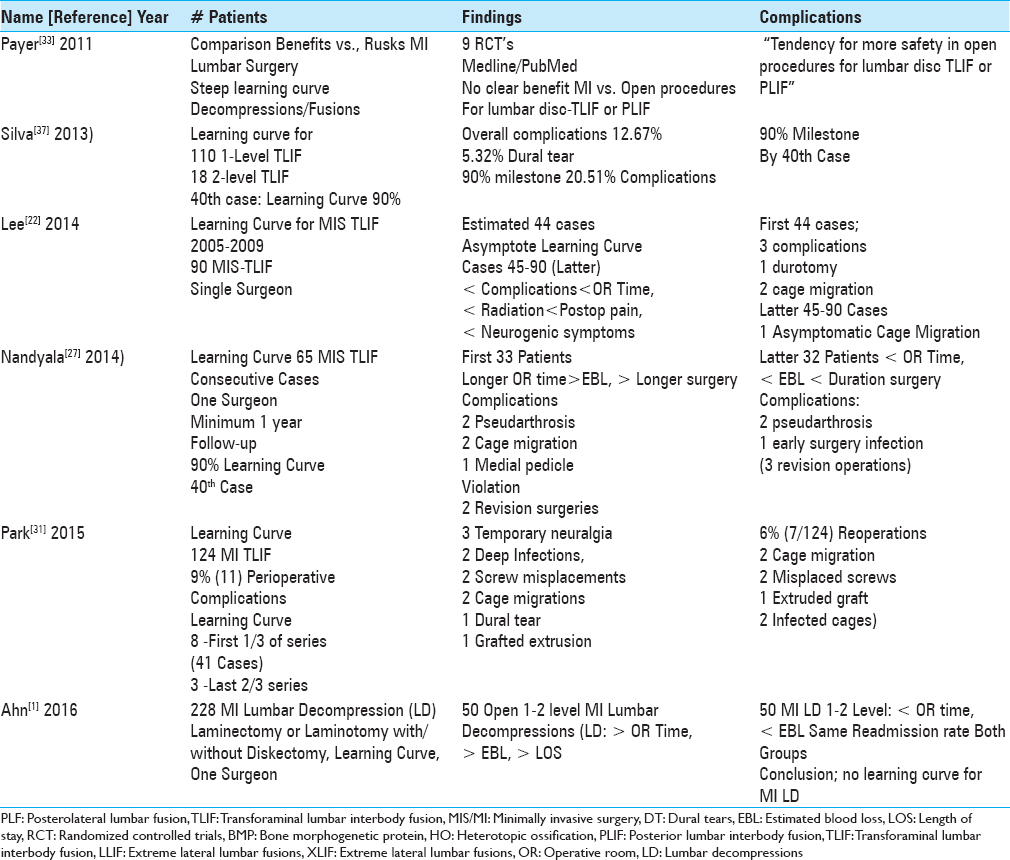
Learning curve for minimally invasive surgery/transforaminal interbody lumbar fusion (MI TLIF)
In 2011, Payer utilized the PubMed and Medline databases and found only 9 RCT that adequately defined the pros and cons of MI lumbar decompressions/stabilization procedures.[
Learning curves: 33–44 cases for minimally invasive transforaminal interbody lumbar fusion (MI TLIF) vs. 0 for minimally invasive decompressions alone
The learning curve for MI TLIF, defined as how many MI TLIF a surgeon needs to perform before becoming technically proficient, was described as involving the first 33–44 cases (e.g. reported in 4 series) [
Increased relative frequency, costs, and reimbursement for instrumented lumbar fusions vs. lumbar laminectomy alone
Several studies documented the increased frequency, costs, and reimbursement rates for instrumented fusion vs. lumbar laminectomy alone addressing degenerative lumbar disease with/without DS.[
DISCUSSION
In this review of the literature, for patients with lumbar degenerative disease/with or without DS, we found lower complication and reoperation rates utilizing laminectomy alone vs. instrumented fusions (e.g., predominantly MI TLIF). For 2 years following Epstein's 137 lumbar multilevel laminectomies without fusions, patients exhibited no new neurological deficits, no infections, 4 (2.9%) had intraoperative CSF fistulas, there were no readmissions, and just 1 patient (0.73%) required a reoperation.[
Based on these data, the choice of procedures to address multilevel degenerative lumbar disease with/without DS should be obvious. Nevertheless, more fusions rather than decompressions alone are increasingly being performed. For example, Bae et al. (Nationwide Inpatient Sample Data) showed that, from 2004 to 2009, decompressions alone decreased from 58.5% to 49.2%, but “simple fusions” (1–2 disc levels/single approach) increased from 21.5% to 31.2%.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ahn J, Iqbal A, Manning BT, Leblang S, Bohl DD, Mayo BC. Minimally invasive lumbar decompression-the surgical learning curve. Spine J. 2016. 16: 909-16
2. Bae HW, Rajaee SS, Kanim LE. Nationwide trends in the surgical management of lumbar spinal stenosis. Spine (Phila Pa 1976). 2013. 38: 916-26
3. Bakhsheshian J, Khanna R, Choy W, Lawton CD, Nixon AT, Wong AP. Incidence of graft extrusion following minimally invasive transforaminal lumbar interbody fusion. J Clin Neurosci. 2016. 24: 88-93
4. Balseiro S, Nottmeier EW. Literature review for infuse: Vertebral osteolysis originating from subchondral cyst end plate defects in transforaminal lumbar interbody fusion using rhBMP-2. Spine J. 2010. 10: e6-10
5. Bernstein DN, Brodell D, Li Y, Rubery PT, Mesfin A. Impact of the Economic Downturn on Elective Lumbar Spine Surgery in the United States: A National Trend Analysis, 2003 to 2013. Global Spine J. 2017. 7: 213-9
6. Bydon M, Macki M, De la Garza-Ramos R, McGovern K, Sciubba DM, Wolinsky JP. Incidence of Adjacent Segment Disease Requiring Reoperation After Lumbar Laminectomy Without Fusion: A Study of 398 Patients. Neurosurgery. 2016. 78: 192-9
7. Chrastil J, Low JB, Whang PG, Patel AA. Complications associated with the use of the recombinant human bone morphogenetic proteins for posterior interbody fusions of the lumbar spine. Spine (Phila Pa 1976). 2013. 38: E1020-7
8. Epstein NE. Pros, cons, and costs of INFUSE in spinal surgery. Surg Neurol Int. 2011. 2: 10-
9. Epstein NE, Schwall GS. Costs and frequency of “off-label” use of INFUSE for spinal fusions at one institution in 2010. Surg Neurol Int. 2011. 2: 115-
10. Epstein NE. Complications due to the use of BMP/INFUSE in spine surgery: The evidence continues to mount. Surg Neurol Int. 2013. 4: S343-52
11. Epstein NE. Adjacent level disease following lumbar spine surgery: A review. Surg Neurol Int. 2015. 6: S591-9
12. Epstein NE. More nerve root injuries occur with minimally invasive lumbar surgery: Let's tell someone. Surg Neurol Int. 2016. 7: S96-S101
13. Epstein NE. Older literature review of increased risk of adjacent segment degeneration with instrumented lumbar fusions. Surg Neurol Int. 2016. 7: S70-6
14. Epstein NE. More nerve root injuries occur with minimally invasive lumbar surgery, especially extreme lateral interbody fusion: A review. Surg Neurol Int. 2016. 7: S83-95
15. Epstein NE. Low reoperation rate following 336 multilevel lumbar laminectomies with noninstrumented fusions. Surg Neurol Int. 2016. 7: S331-6
16. Epstein NE. Tisseel's Impact On Hemostasis For 2-3 and 4-6 Level Lumbar Laminectomies. Surg Neurol Int. 2017. 8: 299-
17. Giorgi H, Prébet R, Delhaye M, Aurouer N, Mangione P, Blondel B. Minimally invasive posterior transforaminal lumbar interbody fusion: One-year postoperative morbidity, clinical and radiological results of a prospective. Orthop Traumatol Surg Resm. 2015. 101: S241-5
18. Høy K, Bünger C, Niederman B, Helmig P, Hansen ES, Li H, Andersen T. Transforaminal lumbar interbody fusion (TLIF) versus posterolateral instrumented fusion (PLF) in degenerative lumbar disorders: A randomized clinical trial with 2-year follow-up. Eur Spine J. 2013. 22: 2022-9
19. Joseph JR, Smith BW, La Marca F, Park P. Comparison of complication rates of minimally invasive transforaminal lumbar interbody fusion and lateral lumbar interbody fusion: A systematic review of the literature. Neurosurg Focus. 2015. 39: E4-
20. Klingler JH, Volz F, Krüger MT1Kogias E, Rölz R, Scholz C. Accidental Durotomy in Minimally Invasive Transforaminal Lumbar Interbody Fusion: Frequency, Risk Factors, and Management. ScientificWorld Journal 2015. 2015. p. 532628-
21. Lad SP, Babu R, Baker AA, Ugiliweneza B, Kong M, Bagley CA. Complications, reoperation rates, and health-care cost following surgical treatment of lumbar spondylolisthesis. J Bone Joint Surg Am. 2013. 6: e162-
22. Lee KH, Yeo W, Soeharno H, Yue WM. Learning curve of a complex surgical technique: Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF). JSDT. 2014. 27: E234-40
23. Liu J, Deng H, Long X, Chen X, Xu R, Liu Z. A comparative study of perioperative complications between transforaminal versus posterior lumbar interbody fusion in degenerative lumbar spondylolisthesis. Eur Spine J. 2016. 25: 1575-80
24. Mannion RJ, Nowitzke AM, Wood MJ. Promoting fusion in minimally invasive lumbar interbody stabilization with low-dose bone morphogenic protein-2-but what is the cost?. Spine J. 2010. 11: 527-33
25. Menger RP, Wolf ME, Kukreja S, Sin A, Nanda A. Medicare payment data for spine reimbursement; important but flawed data for evaluating utilization of resources. Surg Neurol Int. 2015. 6: S391-7
26. Mroz TE, Wang JC, Hashimoto R, Norvell DC. Complications related to osteobiologics use in spine surgery: A systematic review. Spine (Phila Pa 1976). 2010. 35: S86-104
27. Nandyala SVFineberg SJ, Pelton M, Singh K. Minimally invasive transforaminal lumbar interbody fusion: One surgeon's learning curve. Spine J. 2014. 14: 1460-5
28. Nixon AT, Smith ZA, Lawton CD, Wong AP, Dahdaleh NS, Koht A. Bilateral neurological deficits following unilateral minimally invasive TLIF: A review of four patients. Surg Neurol Int. 2014. 5: S317-24
29. Norton RP, Bianco K, Klifto C, Errico TJ, Bendo JA. Degenerative Spondylolisthesis: An Analysis of the Nationwide Inpatient Sample Database. Spine (Phila Pa 1976). 2015. 40: 1219-27
30. Owens K, Glassman SD, Howard JM, Djurasovic M, Witten JL, Carreon LY. Perioperative complications with rhBMP-2 in transforaminal lumbar interbody fusion. Eur Spine J. 2011. 20: 612-7
31. Park Y, Lee SB, Seok SO, Jo BW, Ha JW. Perioperative surgical complications and learning curve associated with minimally invasive transforaminal lumbar interbody fusion: A single-institute experience. Clin Orthop Surg. 2015. 7: 91-6
32. Patil CG, Sarmiento JM, Ugiliweneza B, Mukherjee D, Nuño M, Liu JC. Interspinous device versus laminectomy for lumbar spinal stenosis: A comparative effectiveness study. Spine J. 2014. 14: 1484-92
33. Payer M. “Minimally invasive” lumbar spine surgery: A critical review. Acta Neurochir (Wien). 2011. 153: 1455-9
34. Saetia K, Phankhongsab A, Kuansongtham V, Paiboonsirijit S. Comparison between minimally invasive and open transforaminal lumbar interbody fusion. J Med Assoc Thai. 2013. 96: 41-6
35. Samanta A, Samanta J. Legal standard of care: A shift from the traditional Bolam test. Clin Med (Lond). 2003. 3: 443-6
36. Schöller K, Alimi M, Cong GT, Christos P, Härtl R. Lumbar Spinal Stenosis Associated With Degenerative Lumbar Spondylolisthesis: A Systematic Review and Meta-analysis of Secondary Fusion Rates Following Open vs Minimally Invasive Decompression. Neurosurgery. 2017. 80: 355-67
37. Silva PS, Pereira P, Monteiro P, Silva PA, Vaz R. Learning curve and complications of minimally invasive transforaminal lumbar interbody fusion. Neurosurg Focus. 2013. 35: E7-
38. Wang J, Zhou Y. Perioperative complications related to minimally invasive transforaminal lumbar fusion: Evaluation of 204 operations on lumbar instability at single center. Spine J. 2014. 14: 2078-84
39. Wong DA, Kumar A, Jatana S, Ghiselli G, Wong K. Neurologic impairment from ectopic bone in the lumbar canal: A potential complication of off-label PLIF/TLIF use of bone morphogenetic protein-2 (BMP-2). Spine J. 2008. 8: 1011-8
40. Wong AP, Smith ZA, Nixon AT, Lawton CD, Dahdaleh NS, Wong RH. Intraoperative and perioperative complications in minimally invasive transforaminal lumbar interbody fusion: A review of 513 patients. J Neurosurg Spine. 2015. 22: 487-95
41. Zhang BF, Ge CY, Zheng BL, Hao DJ. Transforaminal lumbar interbody fusion versus posterolateral fusion in degenerative lumbar spondylosis: A meta-analysis. Medicine (Baltimore). 2016. 95: e4995-
42. Zygourakis CC, Liu CY, Wakam G, Moriates C, Boscardin C, Ames CP. Geographic and Hospital Variation in Cost of Lumbar Laminectomy and Lumbar Fusion for Degenerative Conditions. Neurosurgery. 2017. 81: 331-40

