

- Department of Neurosurgery, Institute of Neurosciences, Max Super speciality hospital, Saket, New Delhi, India
- Department of Pathology, Institute of Neurosciences, Max Super speciality hospital, Saket, New Delhi, India
Correspondence Address:
Rohit Bansil
Department of Neurosurgery, Institute of Neurosciences, Max Super speciality hospital, Saket, New Delhi, India
DOI:10.4103/sni.sni_466_16
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Rohit Bansil, Bipin S. Walia, Zahid Khan, Andleeb Abrari. Metastasis to a spinal meningioma. 05-Jun-2017;8:102
How to cite this URL: Rohit Bansil, Bipin S. Walia, Zahid Khan, Andleeb Abrari. Metastasis to a spinal meningioma. 05-Jun-2017;8:102. Available from: http://surgicalneurologyint.com/surgicalint-articles/metastasis-to-a-spinal-meningioma/
Date of Submission
27-Nov-2016
Date of Acceptance
06-Apr-2017
Date of Web Publication
05-Jun-2017
Abstract
Background:Metastasis of one cancer to another is rare. Here, we report a spinal meningioma that was infiltrated by metastatic deposits from another cancer.
Case Description:A 62-year-old male presented with a progressive spastic paraparesis. Magnetic resonance (MR) imaging of the spine suggested a well-defined intradural extramedullary (IDEM) T8 mass in the dorsal spinal canal. When excised, it proved histologically to be a meningothelial meningioma infiltrated by metastatic deposits from an adenocarcinoma.
Conclusion:Tumor to tumor metastasis rarely occurs, and meningioma, owing to its biological character and increased vascularity, is one of the most common recipients of a metastases from other lesions.
Keywords: Meningioma, metastasis, spinal, tumour to tumour
INTRODUCTION
Tumor to tumor metastases are rare. Of the various central nervous system (CNS) tumors, meningiomas are the most common recipients of metastases from other primary cancers in part due to their increased vascularity. Here, we report a patient with multifocal metastatic disease who underwent surgery for excision of dorsal intradural extramedullary lesion at the T8 level. Pathologically, it proved to be a meningothelial meningioma infiltrated by metastatic adenocarcinoma.
CASE REPORT
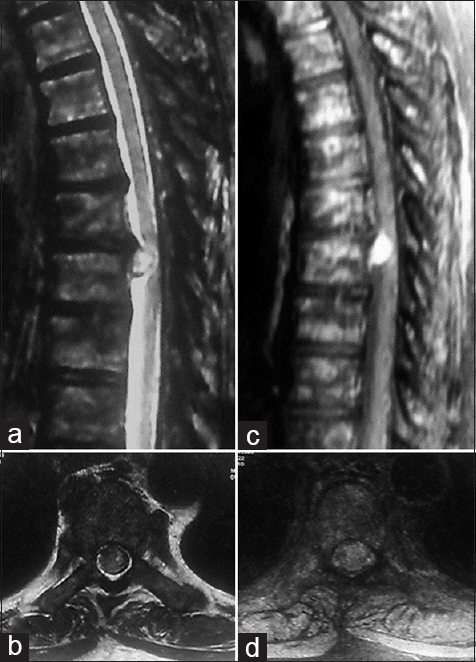
A 62-year-old male presented with 5-month history of progressive paraparesis of the lower extremities (Medical Research council: MRC grade 1/5) without sensory deficits or bladder/bowel involvement. The magnetic resonance (MR) study of the thoracic spine showed a well-defined, ventrally located, intradural extramedullary mass that enhanced heterogeneously with contrast at the T8 spinal level. In addition, it was accompanied by multiple sclerotic lesions consistent with multifocal metastatic disease [
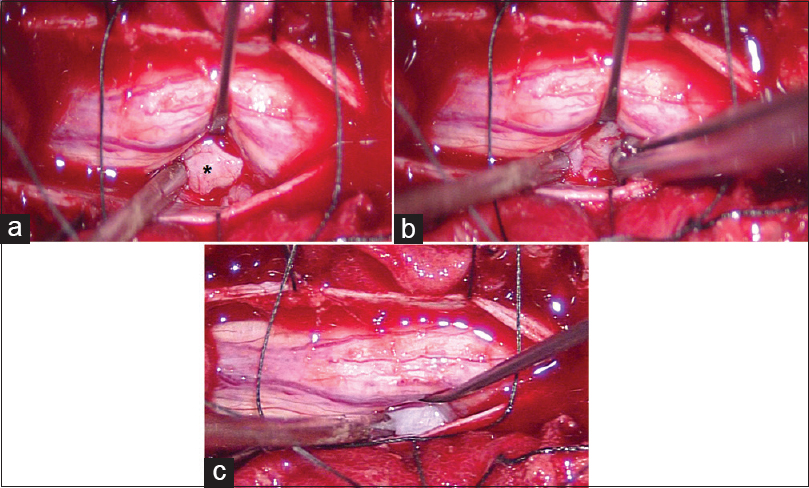
Although no primary cancer was not found, positron emission tomography (PET) scan showed multiple skeletal, thyroid, mediastinal, and lymph node metastases. A complete surgical excision of the T8 extramedullary ventral lesion was performed; it was very firm and adherent to the dura [
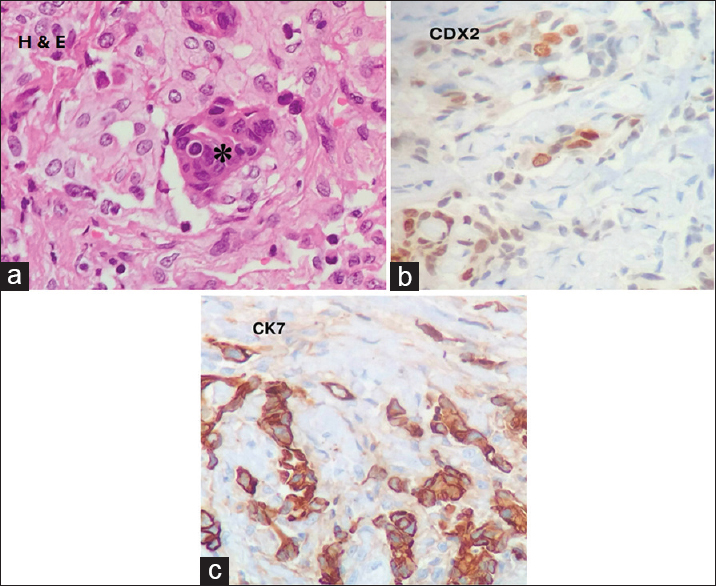
Histopathologically, the mass consisted of both a meningothelial meningioma and diffuse metastatic deposits of a poorly differentiated adenocarcinoma arranged in nests and cords with microacinar structure [Figure
DISCUSSION
Tumor to tumor metastases, first described by Fried in 1930, are rare, with a little over 100 cases reported in the literature.[
Meningiomas are the most common recipients of metastatic lesions largely due to the clinical and biological characteristics of meningiomas (e.g., hypervascularity, high collagen and lipid content, and a slow growth rate).[
Here, the MR scan documented a meningioma that uniformly enhanced with contrast while the multifocal metastases were hypointense. In another series of patients with two such lesions, the MR findings were similar.[
The histopathological examination demonstrated metastatic deposits within the rim of the host tumor; adenocarcinoma most likely spread from the gastrointestinal (GI) tract but no primary lesion could be identified. Spinal metastasis from an unknown primary have been rarely reported.[
The treatment of choice in this case was complete surgical excision of the tumor with appropriate adjuvant therapy. In general, the prognosis for such combined lesions would depend mostly on the nature of the primary tumor.
CONCLUSION
Tumor to tumor metastases are rare and meningiomas, owing to their biological character and increased vascularity, are one of the most common recipients of a metastases from other lesions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Campbel LV, Gilbert E, Chamberlain CR, Watne AL. Metastasis of cancer to cancer. Cancer. 1968. 3: 635-43
2. Lee A, Wallace C, Rewcastle B, Sutherland G. Metastasis to meningioma. Am J Neuroradiol. 1998. 19: 1120-2
3. Moertel CG, Reitemeier RJ, Schutt AJ, Hahn RG. Treatment of the patient with adenocarcinoma of unknown origin. Cancer. 1972. 30: 1469-72
4. Moody P, Murtagh K, Piduru S, Brem S, Murtagh R, Rojiani AM. Tumour-to-tumour metastasis: Pathology and neuroimaging considerations. Int J Clin Exp Pathol. 2012. 5: 367-73
5. Pamphlett R. Carcinoma metastasis to meningioma. J Neurol Neurosurg Psychiatry. 1984. 47: 561-3

