

- Department of Ortho-Spine Surgery, Sir Ganga Ram Hospital, New Delhi, India
Correspondence Address:
Mukesh Kumar Haritwal
Department of Ortho-Spine Surgery, Sir Ganga Ram Hospital, New Delhi, India
DOI:10.4103/sni.sni_315_18
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Mukesh Kumar Haritwal, Shankar Acharya, Kashmiri Lal Kalra, Rupinder Chahal, Nikhil Jain, Nitin Adsul. Odontoid fracture with missed diagnosis of Transverse Atlantal Ligament (TAL) injury resulting in late-onset instability. 28-Nov-2018;9:240
How to cite this URL: Mukesh Kumar Haritwal, Shankar Acharya, Kashmiri Lal Kalra, Rupinder Chahal, Nikhil Jain, Nitin Adsul. Odontoid fracture with missed diagnosis of Transverse Atlantal Ligament (TAL) injury resulting in late-onset instability. 28-Nov-2018;9:240. Available from: http://surgicalneurologyint.com/surgicalint-articles/9094/
Date of Submission
13-Sep-2018
Date of Acceptance
11-Oct-2018
Date of Web Publication
28-Nov-2018
Abstract
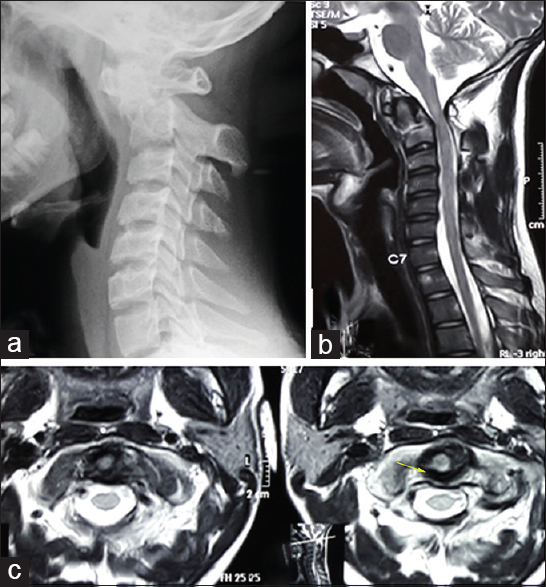
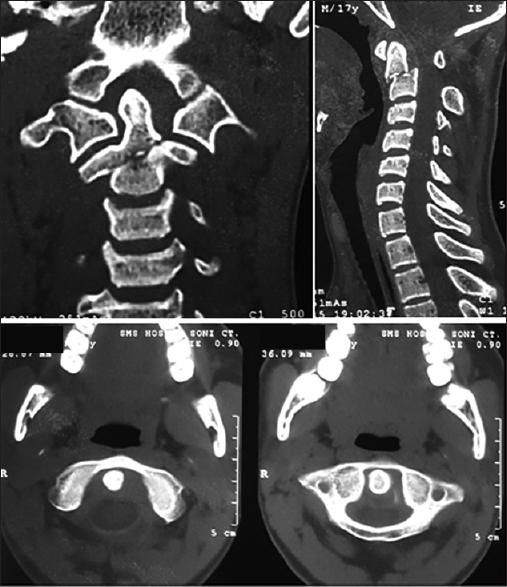
Background:Concurrent injuries to both the odontoid and transverse atlantal ligament are rare and can be easily missed. Failure to diagnose both lesions potentially leads to the late onset of sagittal plane instability and acute myelopathy. Here, we present a patient with an odontoid fracture whose transverse atlantal ligament (TAL) injury was originally missed on magnetic resonance imaging (MRI) and computed tomography (CT) scans. He later developed atlantoaxial instability requiring surgery.
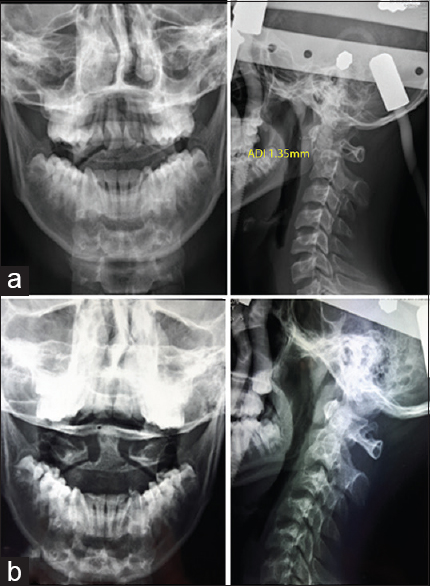
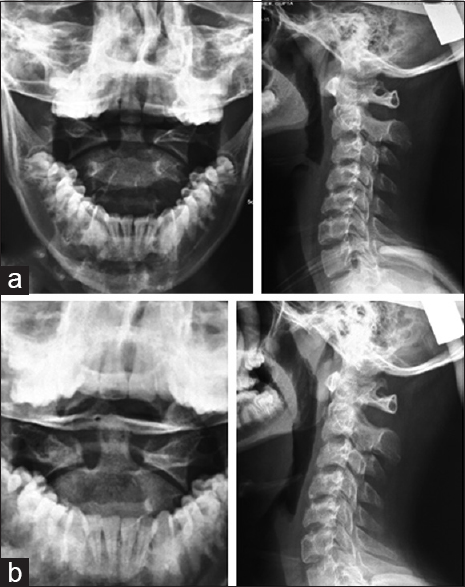
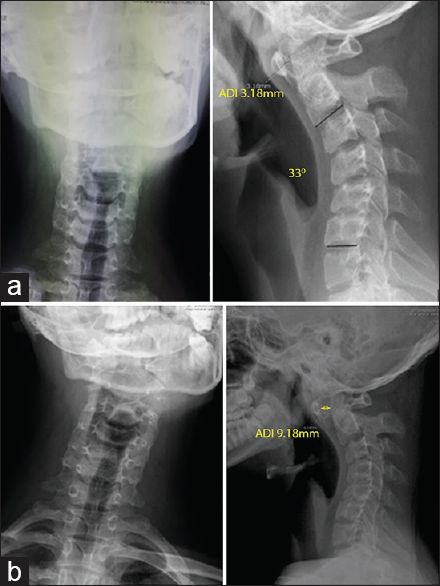
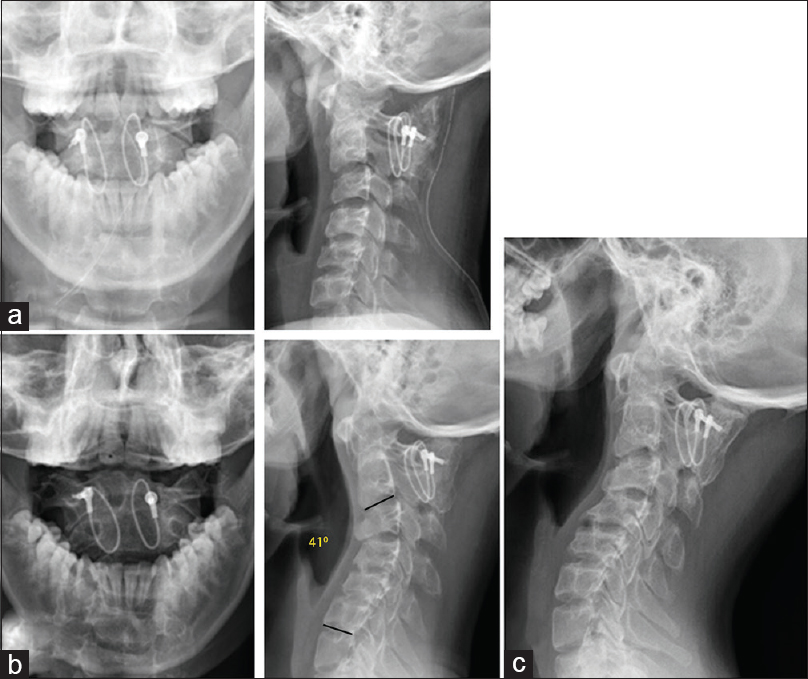
Case Description:A 17-year-old male presented with neck pain, restricted cervical range of motion, but a normal neurological exam following a motor vehicle accident. The original X-rays showed a moderately displaced type-3 odontoid fracture. Additional MRI and CT scans excluded ligamentous injury, and he was initially treated with 13 weeks of halo vest immobilization. Radiographs 5 months later showed an enlarged atlanto-dens interval (e.g., >3 mm); the diagnosis of an odontoid fracture with an accompanying TAL injury was established, following which the patient successfully underwent a posterior C1–C2 fusion.
Conclusion:Odontoid fractures require strict clinical and radiographic (X-ray, MRI, CT) surveillance to help rule out accompanying TAL injuries that may warrant surgical intervention.
Keywords: Atlantoaxial instability, odontoid, transverse atlantal ligament injury
INTRODUCTION
C2 fractures account for 20% of all cervical spine injuries, while odontoid fractures comprise 50% of these injuries.[
CASE REPORT
A 17-year-old male presented 4 days following a motor vehicle accident with neck pain, restricted range of motion, but neurologically intact. X-rays revealed a moderately displaced Anderson & D’ Alonzo type-3 odontoid fracture; however, the atlanto-dens interval (ADI) was maintained (e.g., excluding sagittal atlantoaxial instability) [
Surgical intervention
The fracture was managed with closed reduction and halo vest immobilization [
DISCUSSION
The delayed diagnosis of a TAL associated with an odontoid fracture is rare. In a retrospective review of 77 odontoid fractures, Sayama et al. concluded that odontoid fractures do not require MRI screening for TAL injury.[
Diagnosis and treatment of C1–C2 instability
Anterior widening of ADI more than 3 mm can be seen on mid-sagittal CT reconstructed images. Perez-Orribo et al. compared the CT and MRI measurements to detect the transverse ligament injury, they concluded that no current CT-based measurements consistently indicated integrity of transverse ligament.[
Most odontoid fractures, except for unreducible type II lesions, can be managed nonoperatively with rigid cervical immobilization. Julian et al. reported class III evidence for the successful conservative treatment of type III odontoid fractures utilizing rigid cervical immobilization (e.g., halo vest).[
CONCLUSION
We recommend screening of odontoid fractures for transverse ligament injury with both MRI and CT. If conservative management is used (e.g., halo device), strict radiographic surveillance is required to look for progressive kyphosis/deformity/instability.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bono CM, Carreras E.editors. Cervical spine fractures and dislocations. Rockwood and Green's Fractures in Adults. Philadelphia, PA: Wolters Kluwer, Lippincott Williams & Wilkins; 2010. p. 1313-77
2. Bransford RJ, Patt JC, Chapman JR, Benzel EC.editors. Odontoid fractures. The Cervical Spine. Philadelphia, PA: Wolters Kluwer, Lippincott Williams & Wilkins; 2012. p. 632-64
3. Debernardi A, D’Aliberti G, Talamonti G, Villa F, Piparo M, Cenzato M. Traumatic (type II) odontoid fracture with transverse atlantal ligament injury: A controversial event. World Neurosurg. 2013. 79: 779-83
4. Huang J, Qian B, Qiu Y, Yu Y, Ni HB. Surgical overreduction and hyperlordotic fusion of C1-C2 joint are associated with cervical sagittal malalignment. Arch Orthop Trauma Surg. 2017. 137: 1631-9
5. Julien TD, Frankel B, Traynelis VC, Ryken TC. Evidence-based analysis of odontoid fracture management. Neurosurg Focus. 2000. 8: e1-
6. Perez-Orribo L, Snyder LA, Kalb S, Elhadi AM, Hsu F, Newcomb AG. Comparison of CT versus MRI measurements of transverse atlantal ligament integrity in craniovertebral junction injuries. Part 1: A clinical study. J Neurosurg Spine. 2016. 24: 897-902
7. Sayama CM, Fassett DR, Apfelbaum RI. The utility of MRI in the evaluation of odontoid fractures. J Spinal Disord Tech. 2008. 21: 524-6
8. Sherekar SK, Yadav YR, Basoor AS, Baghel A, Adam N. Clinical implications of alignment of upper and lower cervical spine. Neurol India. 2006. 54: 264-7
9. Tay BK, Eismont FJ.editors. Injuries of the upper cervical spine. Rothman-Simeone. The Spine. Philadelphia, PA: Saunders/Elsevier; 2011. p. 1307-12

