

- Department of Neurosurgery, Rasool Akram Hospital, Tehran, Iran
Correspondence Address:
Morteza Taheri
Department of Neurosurgery, Rasool Akram Hospital, Tehran, Iran
DOI:10.4103/sni.sni_93_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Naderafshar Fereydonyan, Morteza Taheri, Farid Kazemi. Recurrent symptomatic vertebral hemangioma during two consecutive pregnancies: Case report and review of the literature. 05-Jun-2017;8:105
How to cite this URL: Naderafshar Fereydonyan, Morteza Taheri, Farid Kazemi. Recurrent symptomatic vertebral hemangioma during two consecutive pregnancies: Case report and review of the literature. 05-Jun-2017;8:105. Available from: http://surgicalneurologyint.com/surgicalint-articles/recurrent-symptomatic-vertebral-hemangioma-during-two-consecutive-pregnancies-case-report-and-review-of-the-literature/
Date of Submission
01-Mar-2017
Date of Acceptance
09-Apr-2017
Date of Web Publication
05-Jun-2017
Abstract
Background:Pregnancy-related changes can exacerbate the symptoms/signs of vertebral hemangiomas. Here, we report a patient who experienced symptomatic vertebral hemangiomas resulting in cord compression during two consecutive pregnancies.
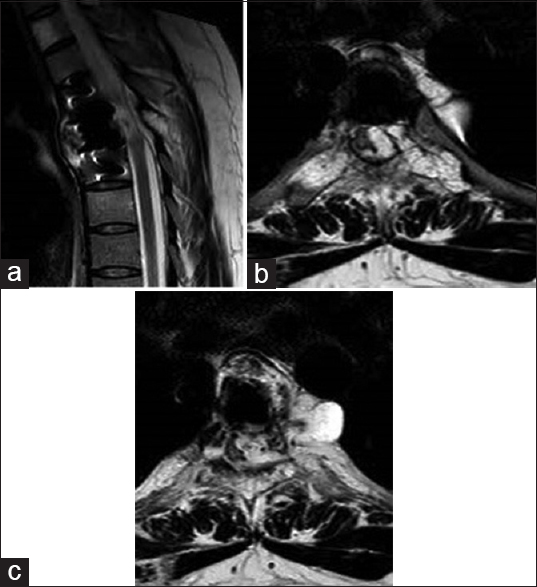
Case Description:A 28-year-old female 34 weeks pregnant, presented with a progressive spastic paraparesis. Magnetic Resonance Imaging (MRI) demonstrated an T5 vertebral body signal change attributed to a hemangioma resulting in cord compression. Following a cesarean section, she had a trans thoracic T5 corpectomy with spinal fusion. Indeed, the histopathology was consistent with a vertebral hemangioma. She fully recovered after this first surgery. However, six years later, she again presented with a spastic paraparesis and sphincter deficit now 29 weeks pregnant. The MR demonstrated cord compression one more at the T5 level attributed to the hemangioma; following a T5 and T6 laminectomy, the left paracentral epidural vascular mass totally resected. Her child was successfully delivered 2 months later at which point she exhibited only mild residual lower limb spasticity.
Conclusion:Patients with known vertebral hemangiomas should be closely monitored during pregnancy as increased growth during these pregnancies may result in progressive spinal cord compression.
Keywords: Pregnancy, symptomatic hemangioma, tumor recurrence, vertebral hemangioma
INTRODUCTION
Pregnancy can exacerbate the growth/presentation of vertebral hemangiomas resulting in increased epidural spinal cord compression. Here, the authors report one patient with two episodes of paraparesis attributed to a T5 hemangioma during two separate pregnancies. The literature concerning 37 other comparable cases of hemangiomas becoming symptomatic during pregnancy were also reviewed.
CASE DESCRIPTION
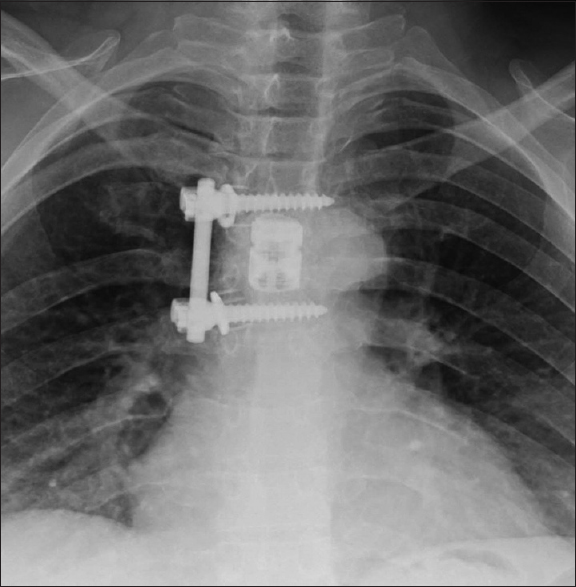
A 28-year-old female in her 34th week of pregnancy presented with progressive paraparesis over a 10-day period. On examination, she was paraplegic with a sensory level and hyperreflexia. The magnetic resonance imaging (MRI) demonstrated a T5 vertebral body hemangioma characterized by an isointense signal on T1 and hyperintense signal on T2-weighted images, which contributed to marked cord compression. After cesarean section, she underwent a transthoracic T5 corpectomy, T4/5 and T5/6 discectomy, and excision of an epidural vascular mass. This was completed by spinal fusion using an expandable cage, screw/rod construct, and bone graft [
DISCUSSION
Vertebral hemangioma is the most common benign spinal neoplasm that occurs in 10–12% of the general population.[
Literature summary
Thirty-seven cases of symptomatic vertebral hemangiomas during pregnancy have been reported [
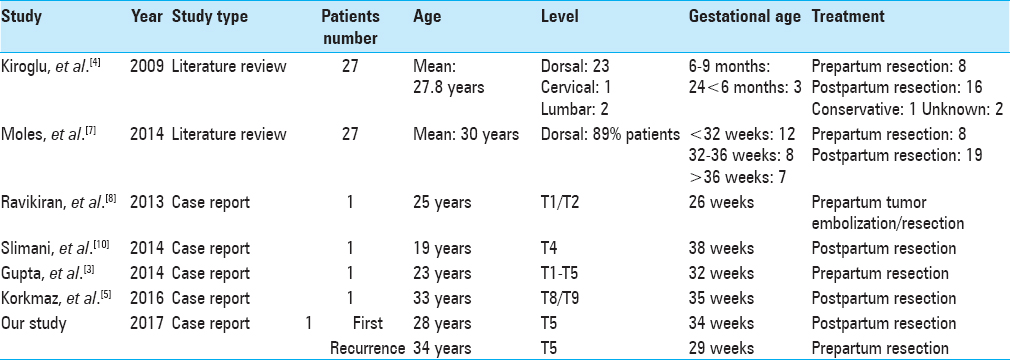
Kiroglu et al. (2009) noted 27 previous case reports about pregnancy-related symptomatic hemangioma in patients averaging 27.8 years of age. They were located in the thoracic spine (23: 17 above T8), cervical spine (1 patient), and the lumbar spine (2 patients).[
Moles et al. (2014) reported 27 cases of pregnancy-related symptomatic hemangiomas; 12 presented at less than 32 weeks, 8 between 32 to 36 weeks, and 7 > 36 weeks. They averaged 30 years of age, and lesions were located mostly in the thoracic spine (89%: 63% in the upper thoracic region).[
Several other studies reported comparable instances of hemangiomas resulting in acute paraparesis at different but latter stages of pregnancy.
Proposed management of vertebral hemangiomas in pregnancy
Chi et al. proposed an algorithm for managing vertebral hemangioma during pregnancy: if the patient is neurologically intact, the management is conservative despite the gestational age. But if the patient has a significant neurological deficit, and the gestational age <32 weeks, antepartum surgery should be performed, whereas a gestational age of >32 weeks, the fetus should first be extracted, and surgery should follow.[
CONCLUSION
It is important to monitor a patient with a vertebral hemangioma for the potential onset of a significant neurological deficit during pregnancy. Hemangiomas can demonstrate increased growth/expansion during pregnancy, and if a neurological deficit acute presents, patients will warrant emergency surgical decompression. Furthermore, despite attempted complete initial resections, recurrent pregnancies may result in recurrent symptomatic hemangiomas.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors declare that they have no conflict of interest, financial or otherwise with any organization.
References
1. Chi JH, Manley GT, Chou D. Pregnancy-related vertebral hemangioma. Case report, review of the literature, and management algorithm. Neurosurg Focus. 2005. 19: E7-
2. Fox MW, Onofrio BM. The natural history and management of symptomatic and asymptomatic vertebral hemangiomas. J Neurosurg. 1993. 78: 36-45
3. Gupta M, Nayak R, Singh H, Khwaja G, Chowdhury D. Pregnancy related symptomatic vertebral hemangioma. Ann Indian Acad Neurol. 2014. 17: 120-2
4. Kiroglu Y, Benek B, Yagci B, Cirak B, Tahta K. Spinal cord compression caused by vertebral hemangioma being symptomatic during pregnancy. Surg Neurol. 2009. 71: 487-92
5. Korkmaz M, Gok M, Cinar C, Guneyli S, Duzgun F, Oran I. Progressive spinal epidural hemangioma in pregnancy. Spine J. 2016. 16: e523-5
6. Lavi E, Jamieson DG, Granat M. Epidural haemangiomas during pregnancy. J Neurol Neurosurg Psychiatry. 1986. 49: 709-12
7. Moles A, Hamel O, Perret C, Bord E, Robert R, Buffenoir K. Symptomatic vertebral hemangiomas during pregnancy. J Neurosurg Spine. 2014. 20: 585-91
8. Ravikiran HG, Harish RP, Ravikumar M, Sandeep N, Roopesh RG, Patil RK. Symptomatic Capillary Hemangioma in Pregnancy: A Rare Case Report of Complete Recovery of Paraparesis with Review of Literature. IJHSR. 2013. 3: 161-6
9. Schwartz TH, Hibshoosh H, Riedel CJ. Estrogen and progesterone receptor-negative T11 vertebral hemangioma presenting as a postpartum compression fracture: Case report and management. Neurosurgery. 2000. 46: 218-21
10. Slimani O, Jayi S, Fdili Alaoui F, Bouguern H, Chaara H, Fikri G. An aggressive vertebral hemangioma in pregnancy: A case report. J Med Case Rep. 2014. 8: 207-
11. Vijay K, Shetty AP, Rajasekaran S. Symptomatic vertebral hemangioma in pregnancy treated antepartum. A case report with review of literature. Eur Spine J. 2008. 17: S299-303

