

- Department of Neurosurgery, Centro Médico “Lic. Adolfo López Mateos”, ISEM. Av Nicolás San Juan S/N, Colonia ex-Hacienda la Magdalena, Toluca, Estado de México, México.
- Radioneurosurgery Unit, Neurological Center, Department of Neurosurgery, National Institute of Neurology and Neurosurgery “Dr. Manuel Velasco Suarez”, Av. Insurgentes Sur No. 3877, La Fama, México.
- American British Cowray Medical Center, Carlos Graef Fernández No. 154, Col. Santa Fe, Cuajimalpa, México City, México.
Correspondence Address:
José Alfonso Franco-Jiménez
Department of Neurosurgery, Centro Médico “Lic. Adolfo López Mateos”, ISEM. Av Nicolás San Juan S/N, Colonia ex-Hacienda la Magdalena, Toluca, Estado de México, México.
DOI:10.25259/SNI-11-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Saúl Solorio-Pineda, Adriana Ailed Nieves-Valerdi, José Alfonso Franco-Jiménez, Guillermo Axayacalt Gutiérrez-Aceves, Luis Manuel Buenrostro-Torres, Milton Inocencio Ruíz-Flores. Retroclival and spinal subdural hematoma after traumatic brain injury - A case report and literature review. 10-May-2019;10:86
How to cite this URL: Saúl Solorio-Pineda, Adriana Ailed Nieves-Valerdi, José Alfonso Franco-Jiménez, Guillermo Axayacalt Gutiérrez-Aceves, Luis Manuel Buenrostro-Torres, Milton Inocencio Ruíz-Flores. Retroclival and spinal subdural hematoma after traumatic brain injury - A case report and literature review. 10-May-2019;10:86. Available from: http://surgicalneurologyint.com/surgicalint-articles/9342/
Date of Submission
09-Jan-2019
Date of Acceptance
07-Feb-2019
Date of Web Publication
10-May-2019
Abstract
Background: Retroclival hematomas are rare and occur mostly in the pediatric population. They are variously attributed to trauma, apoplexy, and vascular lesions. With motor vehicle accidents (MVAs), the mechanism of traumatic injury is forced flexion and extension. There may also be associated cervical spinal and/or clivus fractures warranting fusion.
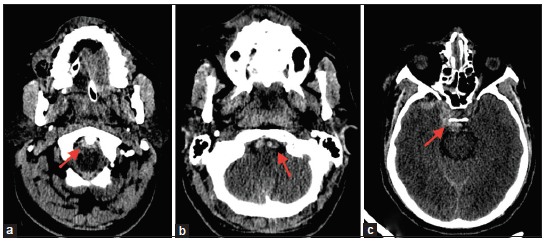
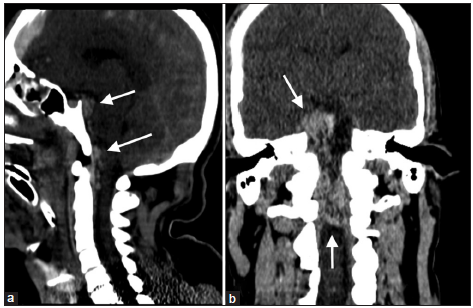
Case Description: A 35-year-old male sustained a traumatic brain injury after a fall of 5 m at work. His Glasgow coma scale (GCS) on admission was 13 (M6V3O4). He had no cranial nerve deficits. The brain computed tomography (CT) showed a retroclival subdural hematoma that extended to the C2 level.
Conclusions: Most retroclival hematomas are attributed to MVAs, and cranial CT and magnetic resonance studies typically demonstrate a combination of posterior fossa hemorrhage with retroclival hematomas (intra or extradural). Patients with retroclival hematomas but high GCS scores on admission usually have better prognoses following traumatic brain injuries attributed to MVA. Notable however is the frequent association with additional cervical and/or craniocervical injuries (e.g. such as odontoid fracture) that may warrant surgery/fusión.
Keywords: Retroclival hematoma, subdural hematoma, traumatic brain injury
INTRODUCTION
Retroclival hematomas are rare, occurring mostly in the pediatric age group.[
CLINICAL CASE
A 35-year-old male sustained a traumatic brain injury (Glasgow coma scale [GCS] of 13) following a fall of 5 m. On admission, he was delirious and had bilateral pupils measuring 3 mm without attendant cranial nerves palsies. The skull X-ray showed a non- displaced right frontotemporal fracture and fractures of the right orbital floor, lateral wall/roof, and nasal bones. The brain computed tomography (CT) documented a posttraumatic subarachnoid hemorrhage, right frontal subdural hematoma, and retroclival subdural hematoma extending to the C2 level with partial collapse of the infratentorial cisterns [
DISCUSSION
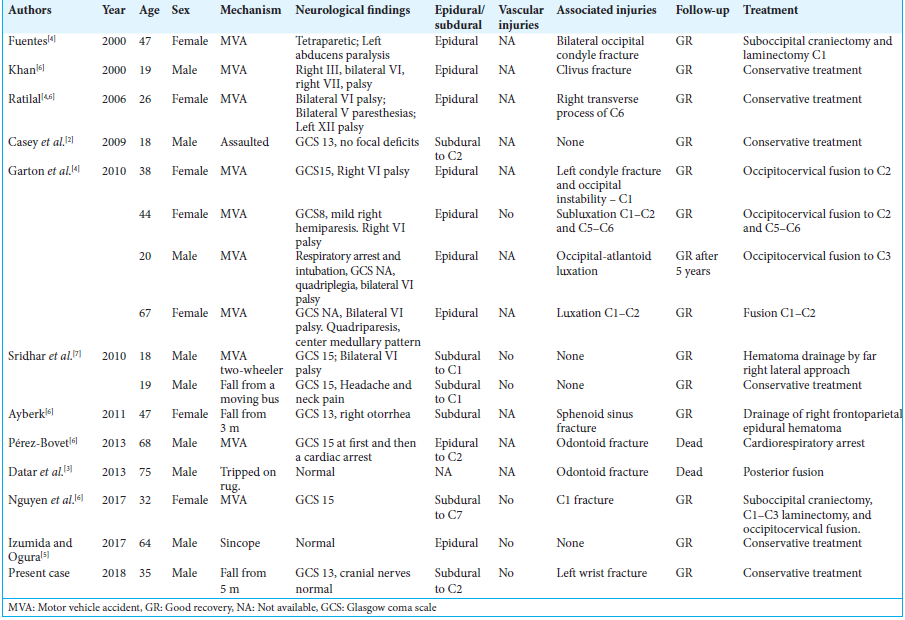
Most retroclival hematomas are attributed to MVAs and generally carry a good prognosis [
In the case presented, the patient had no cranial nerve palsies and required no surgery despite CT-documented posttraumatic subarachnoid hemorrhage, a right frontal subdural hematoma, a retroclival subdural hematoma extending to the C2 level, and partial collapse of the infratentorial cisterns. Notably, he was fully intact on discharge 11 days later.
CONCLUSIONS
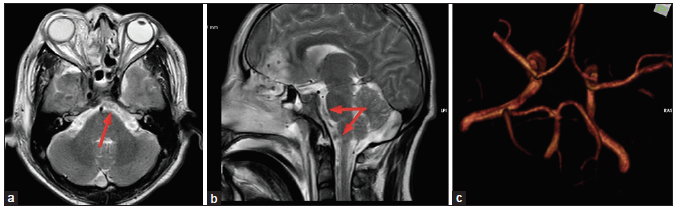
Retroclival hematomas are rare in adults. These patients should undergo both CT and MR studies to document the location/extent of these hematomas along with other cranial/cervical pathology (e.g., hematomas, fractures, and ligamentous injuries). The majority of patients do well without surgical intervention; only a few warrant posterior fossa decompression for clot evacuation with/without cervical and/or craniocervical fusion.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
References
1. Ahn ES, Smith ER. Acute clival and spinal subdural hematoma with spontaneous resolution: Clinical and radiographic correlation in support of a proposed pathophysiological mechanism. Case report. J Neurosurg. 2005. 103: 175-9
2. Casey D, Chaudhary BR, Leach PA, Herwadkar A, Karabatsou K. Traumatic clival subdural hematoma in an adult. J Neurosurg. 2009. 110: 1238-41
3. Datar S, Daniels D, Wijdicks EF. A major pitfall to avoid: Retroclival hematoma due to odontoid fracture. Neurocrit Care. 2013. 19: 206-9
4. Garton HJ, Gebarski SS, Ahmad O, Trobe JD. Clival epidural hematoma in traumatic sixth cranial nerve palsies combined with cervical injuries. J Neuroophthalmol. 2010. 30: 18-25
5. Izumida T, Ogura K. Minor traumatic retroclival epidural haematoma in an adult. BMJ Case Rep. 2017. 2017:
6. Nguyen HS, Shabani S, Lew S. Isolated traumatic retroclival hematoma: Case report and review of literature. Childs Nerv Syst. 2016. 32: 1749-55
7. Sridhar K, Venkateswara PG, Ramakrishnaiah S, Iyer V. Posttraumatic retroclival acute subdural hematoma: Report of two cases and review of literature. Neurol India. 2010. 58: 945-8

