

- Department of Neurosurgery, Mito Brain Heart Center, Mito, Ibaraki, Japan.
DOI:10.25259/SNI_262_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Taro Yanagawa, Yoichi Harada, Toru Hatayama, Takuji Kono. Rupture immediately after growth of unruptured intracranial aneurysms during follow-up. 23-Aug-2019;10:164
How to cite this URL: Taro Yanagawa, Yoichi Harada, Toru Hatayama, Takuji Kono. Rupture immediately after growth of unruptured intracranial aneurysms during follow-up. 23-Aug-2019;10:164. Available from: http://surgicalneurologyint.com/surgicalint-articles/9593/
Date of Submission
25-Apr-2019
Date of Acceptance
19-Jun-2019
Date of Web Publication
23-Aug-2019
Abstract
Background: The annual rupture rate of small unruptured intracranial aneurysms (UIAs)
Case Description: A 1-mm right middle cerebral artery aneurysm was incidentally found in a 63-year-old woman. Preventive surgery was planned because the aneurysm grew rapidly; however, the aneurysm ruptured preoperatively. A 68-year-old woman had a small (4 mm) aneurysm at the left internal carotid-posterior communicating artery. The aneurysm grew rapidly after many years. Several hours after magnetic resonance imaging was performed, she presented to the hospital with loss of consciousness, and a diagnosis of subarachnoid hemorrhage due to the ruptured aneurysm was made.
Conclusion: UIAs that rapidly increase during follow-up may be regarded as impending ruptured aneurysms.
Keywords: Impending ruptured aneurysm, Magnetic resonance imaging, Subarachnoid hemorrhage, Unruptured intracranial aneurysm
INTRODUCTION
Research on unruptured intracranial aneurysms (UIAs) has progressed and its natural history has recently been better defined according to multiple prospective studies. Due to the increasing use of magnetic resonance imaging (MRI) for various symptoms, asymptomatic small UIAs are being detected more frequently. The annual rupture rate of small UIAs <5 mm is generally low and small UIAs are often treated conservatively. Aneurysm growth during follow-up is reportedly associated with a high rupture risk.[
CASE DESCRIPTIONS
Case 1
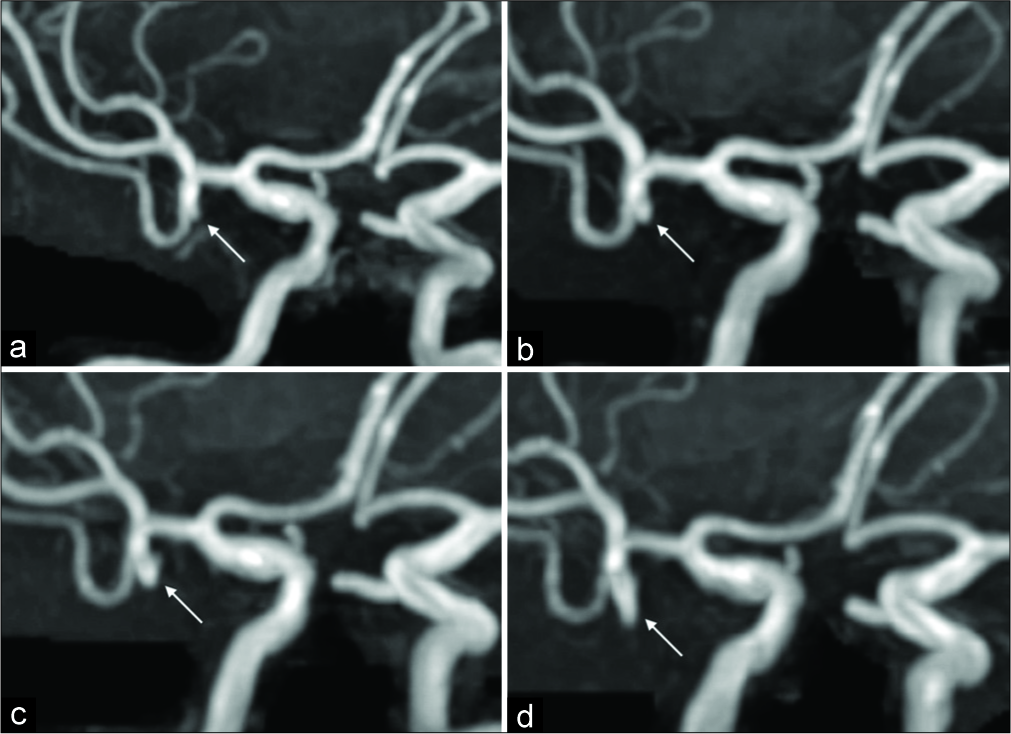
A 1-mm right middle cerebral artery aneurysm was incidentally revealed in a 63-year-old woman on MRI [
Case 2
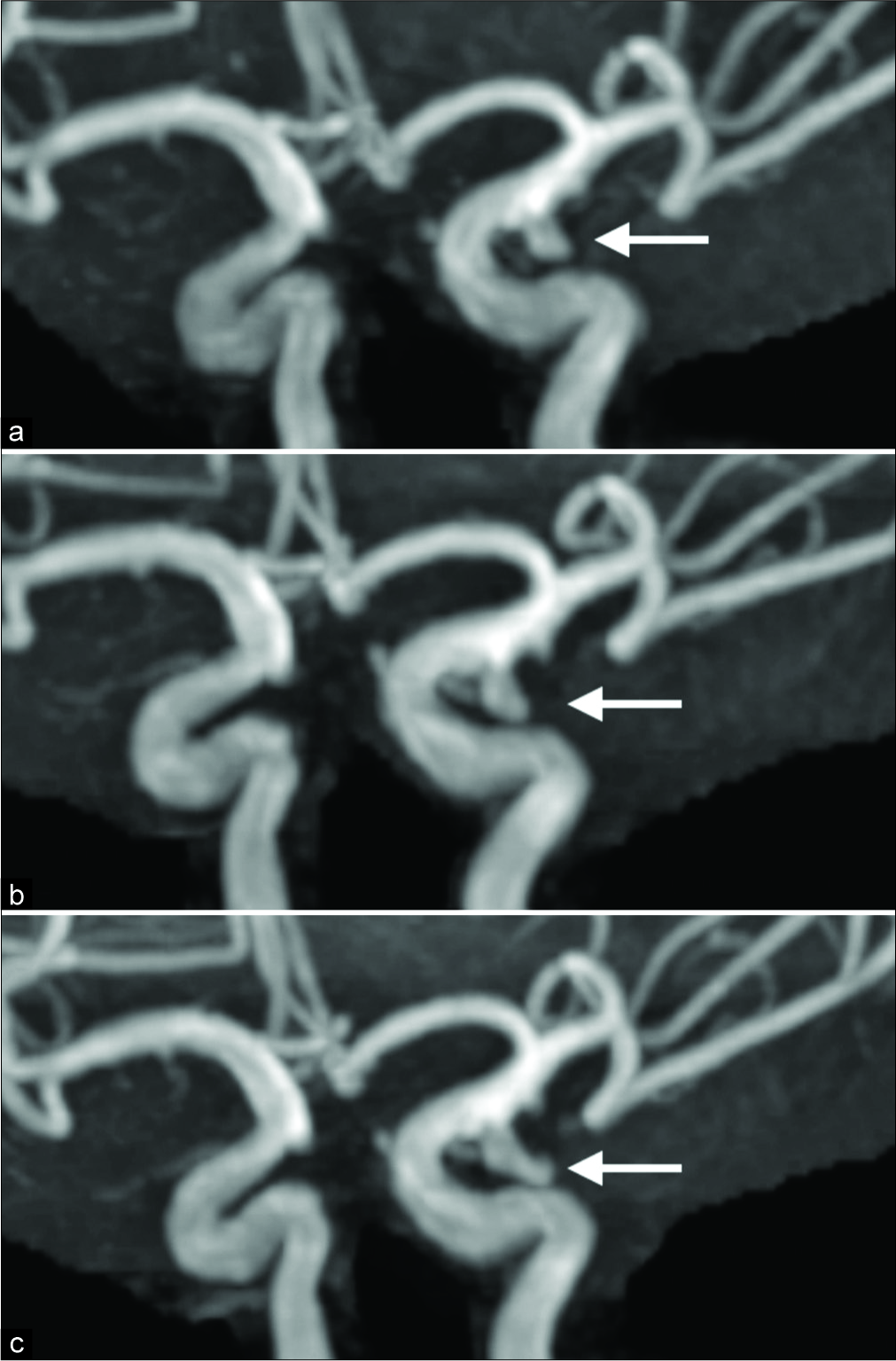
A 68-year-old woman >had no significant medical history; however, MRI performed during a routine health check-up incidentally revealed a small aneurysm (4 mm) at the left internal carotid-posterior communicating artery. Subsequent MRIs performed every 6 or 12 months revealed no significant changes in the aneurysm size [
DISCUSSION
The present study highlights two important clinical issues. First, UIAs that show rapid growth during follow-up may rupture within a short period. During observation, UIAs must be compared against the initial image as well as the previous image. When UIAs sized ≤5 mm are detected incidentally, follow-up may be appropriate due to the low rupture rate (for example, 0.54%/year in the SUAVe study and 0.36%/year in the UCAS Japan report).[
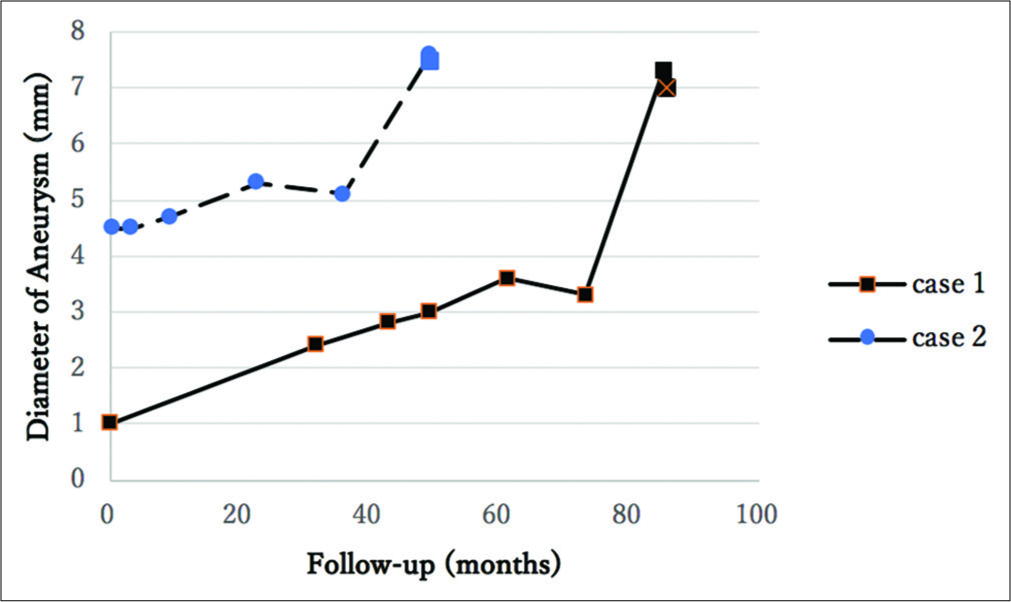
In both cases 1 and 2, the growth rate of UIAs just before rupture was 2.24 and 3.97 mm/year, respectively; this rate was much more rapid growth than that reported by Juvela.[
Second, during observation, the UIAs must be compared with the initial and previous images. When UIAs are followed closely, it seems that MRI is often performed approximately once a year and slow growth may be missed when compared with only the previous image. When the growth of UIAs was ≤1 mm on MRI, the judgment was difficult. However, comparison with several prior MRI images could have shown a clear growth. For such patients, it is recommended that a request for direct comparison with the results of the initial diagnostic exam be included in the instructions provided to the radiologist for the follow-up magnetic resonance angiography/CTA. The previous studies have reported that UIAs have the highest rate of rupture immediately after aneurysm formation and that the rate gradually decreases subsequently.[
CONCLUSION
UIAs that show rapid growth during follow-up can rupture within a short period. During observation, UIAs must be compared against the initial and previous images. UIAs that show rapid growth during follow-up could be regarded as impending ruptured aneurysms even if they are asymptomatic. Hence, the urgency of treatment for such aneurysms should be carefully determined. Further reports should be accumulated to examine the rate of growth of the ruptured aneurysm during follow-up.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Inoue T, Shimizu H, Fujimura M, Saito A, Tominaga T. Annual rupture risk of growing unruptured cerebral aneurysms detected by magnetic resonance angiography. J Neurosurg. 2012. 117: 20-5
2. Juvela S. Growth and rupture of unruptured intracranial aneurysms. J Neurosurg. 2018. 1: 1-9
3. Mehan WA, Romero JM, Hirsch JA, Sabbag DJ, Gonzalez RG, Heit JJ. Unruptured intracranial aneurysms conservatively followed with serial CT angiography: Could morphology and growth predict rupture?. J Neurointerv Surg. 2014. 6: 761-6
4. Mitchell P, Jakubowski J. Estimate of the maximum time interval between formation of cerebral aneurysm and rupture. J Neurol Neurosurg Psychiatry. 2000. 69: 760-7
5. Sonobe M, Yamazaki T, Yonekura M, Kikuchi H. Small unruptured intracranial aneurysm verification study: SUAVe study, Japan. Stroke. 2010. 41: 1969-77
6. UCAS Japan Investigators, Morita A, Kirino T, Hashi K, Aoki N, Fukuhara S. The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med. 2012. 366: 2474-82
7. Villablanca JP, Duckwiler GR, Jahan R, Tateshima S, Martin NA, Frazee J. Natural history of asymptomatic unruptured cerebral aneurysms evaluated at CT angiography: Growth and rupture incidence and correlation with epidemiologic risk factors. Radiology. 2013. 269: 258-65
8. Wermer MJ, van der Schaaf IC, Algra A, Rinkel GJ. Risk of rupture of unruptured intracranial aneurysms in relation to patient and aneurysm characteristics: An updated meta-analysis. Stroke. 2007. 38: 1404-10

