

- Department of Neurosurgery, University of Illinois at Chicago, Chicago, Illinois, USA
Correspondence Address:
Ali Alaraj
Department of Neurosurgery, University of Illinois at Chicago, Chicago, Illinois, USA
DOI:10.4103/sni.sni_430_17
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nauman S. Chaudhry, Denise Brunozzi, Sophia F. Shakur, Fady T. Charbel, Ali Alaraj. Ruptured posterior cerebral artery aneurysm presenting with a contralateral cranial nerve III palsy: A case report. 01-Mar-2018;9:52
How to cite this URL: Nauman S. Chaudhry, Denise Brunozzi, Sophia F. Shakur, Fady T. Charbel, Ali Alaraj. Ruptured posterior cerebral artery aneurysm presenting with a contralateral cranial nerve III palsy: A case report. 01-Mar-2018;9:52. Available from: http://surgicalneurologyint.com/surgicalint-articles/ruptured-posterior-cerebral-artery-aneurysm-presenting-with-a-contralateral-cranial-nerve-iii-palsy-a-case-report/
Date of Submission
16-Nov-2017
Date of Acceptance
09-Jan-2018
Date of Web Publication
01-Mar-2018
Abstract
Background:Posterior cerebral artery aneurysms can frequently present with an ipsilateral cranial nerve III palsy.
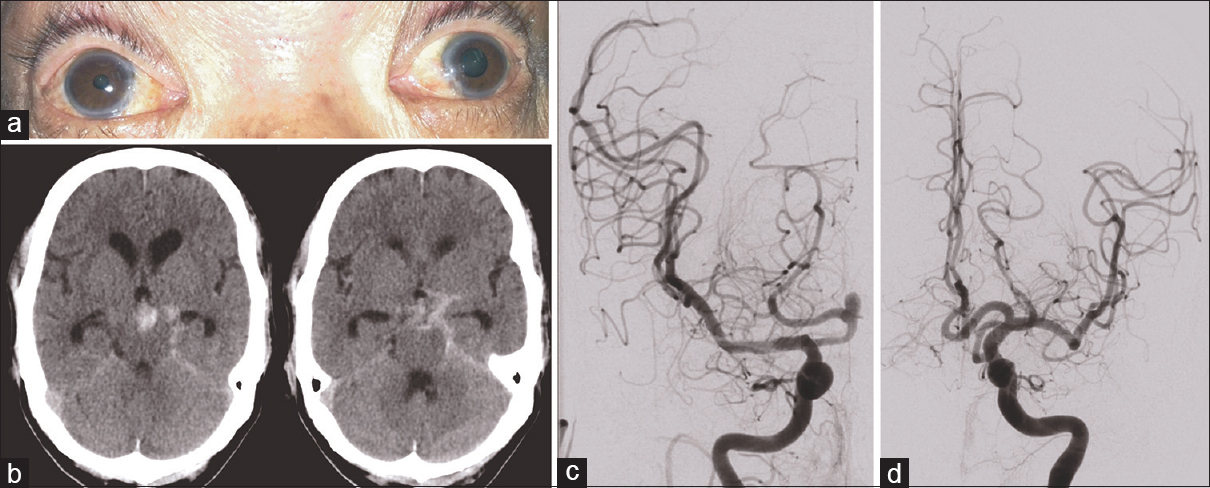
Case Description:We report the first case of a posterior cerebral artery aneurysm associated with a contralateral cranial nerve III palsy. A 64-year-old male presented with acute subarachnoid hemorrhage, Hunt and Hess grade 3, and a left-sided fixed and dilated pupil. Computed tomography scan showed hemorrhage, mainly within the left basal cisterns. Digital subtraction angiography revealed a right-sided P1–P2 junction aneurysm.
Conclusions:This case demonstrates that, although the neurological exam can help pinpoint the location of a lesion, false localizing signs should be recognized.
Keywords: Cerebral aneurysm, cranial nerve III, oculomotor nerve, posterior cerebral artery, posterior communicating artery, subarachnoid hemorrhage
INTRODUCTION
Cranial nerve III (CN III) palsy from a posterior communicating artery (PCoA), posterior cerebral artery (PCA), or superior cerebellar artery aneurysm is a well-established phenomenon.[
CASE PRESENTATION
Clinical presentation
A 64-year-old Cantonese male, with no significant past medical history, was transferred to our institution with acute subarachnoid hemorrhage, Hunt and Hess grade 3, and Fisher grade 4. Upon arrival, Glasgow coma scale score was 8 and so he was intubated. His left pupil was also fixed and measured 5 mm [
Aneurysm treatment
The aneurysm was successfully treated with balloon-assisted coil embolization via the right PCoA. A small neck remnant was noted, and hence 6 weeks after presentation, the patient underwent pipeline stent placement within the right PCA across the aneurysm neck.
Clinical course
The patient was managed in our neurosurgical intensive care unit for approximately 2 weeks and on the floor for 4 weeks. He required two additional angiograms for vasospasm treatment with intraarterial verapamil. He also required shunting, tracheostomy, and percutaneous endoscopic gastrostomy tube. However, the tracheostomy was decannulated and he was transitioned to oral intake by the time of discharge. He was discharged home and was awake, following commands, moving all extremities with full strength, and had near resolution of his CN III palsy with the left pupil 1 mm larger than the right pupil.
DISCUSSION
The finding of pupil dilatation is most commonly associated with ipsilateral lesions such as hemorrhage, uncal herniation, or cerebral aneurysms of the PCoA, PCA, or SCA that cause external compression on the parasympathetic efferent fibers of CN III.
Causes of a CN III palsy contralateral to the lesion are still unclear and have been attributed to aberrant anatomy of CN III and rotational forces on the brainstem.[
In our patient, initial imaging [
CONCLUSION
We report the first case of a posterior cerebral artery aneurysm associated with a contralateral CN III palsy. Although the neurological examination plays a critical role for operative planning, false localizing signs need to be considered prior to any definitive management plan.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Brigui M, Chauvet D, Clarençon F, Degos V, Sourour NA, Nouet A. Recovery from oculomotor nerve palsy due to posterior communicating artery aneurysms: Results after clipping versus coiling in a single-center series. Acta Neurochir (Wien). 2014. 156: 879-84
2. Browder J. A Resumé of the Principal Diagnostic Features of Subdural Hematoma. Bull N Y Acad Med. 1943. 19: 168-76
3. Chen R, Sahjpaul R, Del Maestro RF, Assis L, Young GB. Initial enlargement of the opposite pupil as a false localising sign in intraparenchymal frontal haemorrhage. J Neurol Neurosurg Psychiatry. 1994. 57: 1126-8
4. Chesnut RM, Gautille T, Blunt BA, Klauber MR, Marshall LE. The localizing value of asymmetry in pupillary size in severe head injury: Relation to lesion type and location. Neurosurgery. 1994. 34: 840-5
5. Chung KH, Chandran KN. Paradoxical fixed dilatation of the contralateral pupil as a false-localizing sign in intraparenchymal frontal hemorrhage. Clin Neurol Neurosurg. 2007. 109: 455-7
6. Fujiwara S, Fujii K, Nishio S, Matsushima T, Fukui M. Oculomotor nerve palsy in patient with cerebral aneurysms. Neurosurg Rev. 1989. 12: 123-32
7. Gassel MM. False localizing signs, A review of the concept and analysis of the occurrence in 250 cases of intracranial meningioma. Arch Neurol. 1961. 4: 526-54
8. Hanse MC, Gerrits MC, van Rooij WJ, Houben MP, Nijssen PC, Sluzewski M. Recovery of posterior communicating artery aneurysm-induced oculomotor palsy after coiling. AJNR Am J Neuroradiol. 2008. 29: 988-90
9. Moon K, Albuquerque FC, Ducruet AF, Crowley RW, McDougall CG. Resolution of cranial neuropathies following treatment of intracranial aneurysms with the Pipeline Embolization Device. JNeurosurg. 2014. 121: 1085-92
10. Pevehouse BC, Bloom WH, McKissock W. Ophthalmologic aspects of diagnosis and localization of subdural hematoma.An analysis of 389 cases and review of the literature. Neurology. 1960. 10: 1037-41

