

- Division of Neurosurgery, University of Missouri, One Hospital Drive, MC314 McHaney Hall, Columbia, Missouri, USA.
DOI:10.25259/SNI-302-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sarah S. Travers, Thorkild V. Norregaard. Spinal cord stimulator failure: Migration of a thoracic epidural paddle to the cervical spine. 25-Jun-2019;10:118
How to cite this URL: Sarah S. Travers, Thorkild V. Norregaard. Spinal cord stimulator failure: Migration of a thoracic epidural paddle to the cervical spine. 25-Jun-2019;10:118. Available from: http://surgicalneurologyint.com/surgicalint-articles/9406/
Date of Submission
11-May-2019
Date of Acceptance
28-May-2019
Date of Web Publication
25-Jun-2019
Abstract
Background: Spinal cord stimulators successfully treat a number of pain syndromes but carry a risk of hardware complications. Here, we present a case of cranial migration of a thoracic epidural paddle to the cervical spine.
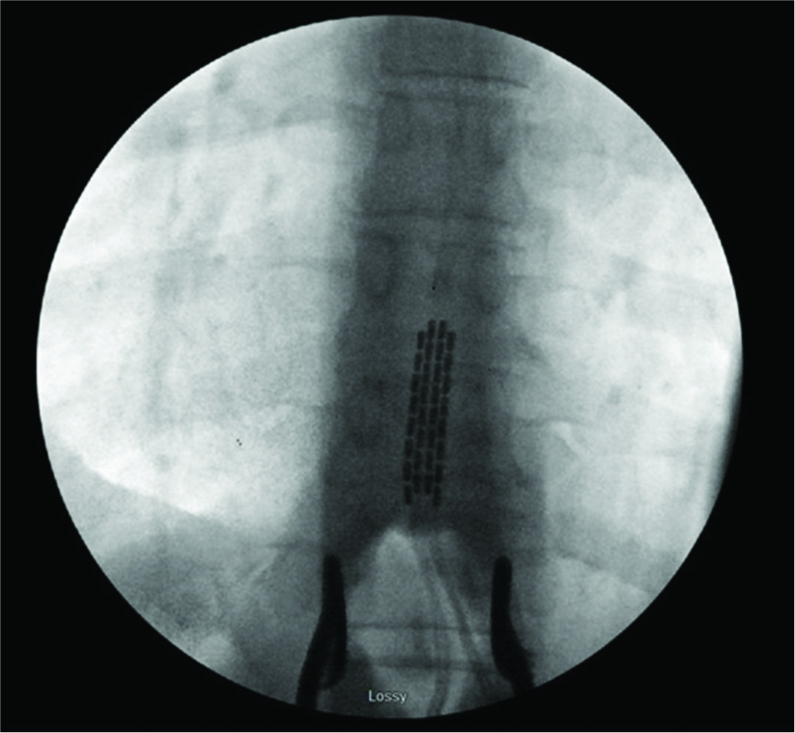
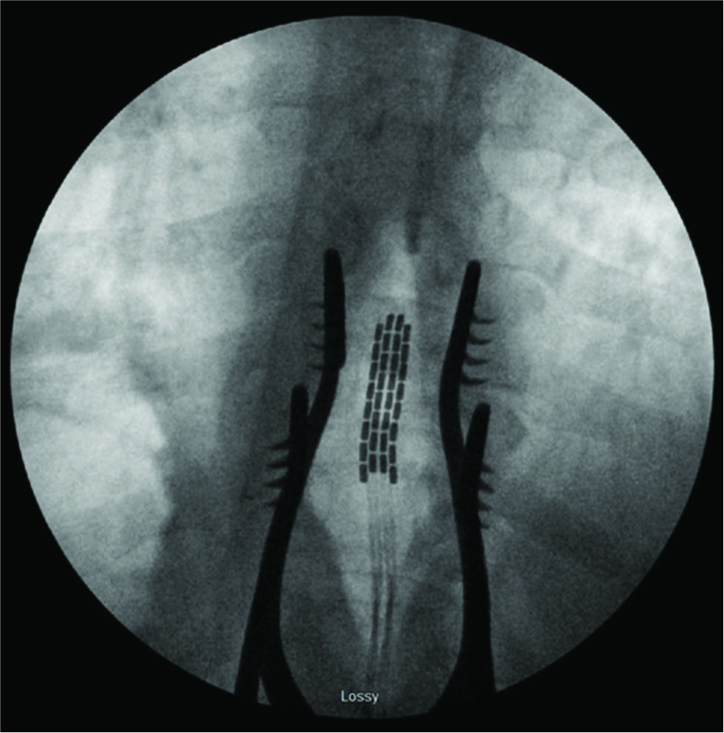
Case Description: A 53-year-old male underwent uncomplicated spinal cord stimulator placement at the T10– T11 with initially favorable results. However, postoperatively, he complained of paresthesias in his arms. An X-ray demonstrated cranial migration of the thoracic epidural paddle to the cervical spine. The stimulator/new paddle was placed again at the T10–T11 level, but the leads were now secured to the caudal lamina utilizing a cranial plating system. The patient subsequently did well without further sequelae.
Conclusions: A thoracic epidural paddle (T10–T11) migrated postoperatively into the cervical spine. It was subsequently removed and replaced into the thoracic region, but the leads were now secured in place with a novel caudal lamina/cranial plating system.
Keywords: Failed back surgery syndrome, Hardware failure, Lead migration, Spinal cord stimulation, Stimulator
INTRODUCTION
Spinal cord stimulation (SCS) is frequently used to treat failed back surgery syndrome, chronic regional pain syndrome, chronic back pain, neuropathy, ischemic pain, and visceral pain. However, this procedure is associated with some risks that include infection, bleeding, spinal cord injury, and hardware complications.[
CASE PRESENTATION
A 53-year-old male underwent a right L4-L5 microdiscectomy and foraminotomy and was discharged home the same day. With no improvement 6 months after surgery, we offered a trial of SCS, and he experienced significant relief from the back and leg pain. Ten days later, we placed an epidural paddle electrode through a T10–T11 laminotomy [

DISCUSSION
Lead migration is one of the most common complications occurring in from 2.1% to 27% out of 5000 patients undergoing SCS.[
CONCLUSIONS
Here, a 53-year-old male demonstrated migration of a thoracic epidural paddle electrode into the cervical spine. This required replacement of the T10–T11 leads and an alternative method of affixing of these leads in place utilizing a craniofacial plating system.
References
1. Eldabe S, Buchser E, Duarte RV. Complications of spinal cord stimulation and peripheral nerve stimulation techniques: A review of the literature. Pain Med. 2016. 17: 325-36
2. Kumar K, Hunter G, Demeria D. Spinal cord stimulation in treatment of chronic benign pain: Challenges in treatment planning and present status, a 22-year experience. Neurosurgery. 2006. 58: 481-96
3. Tomycz ND, Cameron J, Whiting DM, Oh MY. Cranial plate anchoring of spinal cord stimulation paddle leads: Technical note. Neurosurgery. 2012. 71: 22-4

