

- Department of Neurosurgery, GMCH, Kozhikode, Kerala, India
- Department of Neuropathology, NIMHANS, Bengaluru, Karnataka, India
Correspondence Address:
Pravin Y. Waykule
Department of Neuropathology, NIMHANS, Bengaluru, Karnataka, India
DOI:10.4103/sni.sni_94_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: M. P. Rajeev, Pravin Y. Waykule, V. M. Pavitharan, B. N. Nandeesh. Spinal epidural capillary hemangioma: A rare case report with a review of literature. 21-Jun-2017;8:123
How to cite this URL: M. P. Rajeev, Pravin Y. Waykule, V. M. Pavitharan, B. N. Nandeesh. Spinal epidural capillary hemangioma: A rare case report with a review of literature. 21-Jun-2017;8:123. Available from: http://surgicalneurologyint.com/surgicalint-articles/spinal-epidural-capillary-hemangioma-a-rare-case-report-with-a-review-of-literature/
Date of Submission
22-Mar-2017
Date of Acceptance
06-May-2017
Date of Web Publication
21-Jun-2017
Abstract
Background:Purely epidural capillary hemangiomas are very rare. There are only 6 such reports.
Case Description:A 50-year-old male presented with a progressive lower extremity paraparesis. Magnetic resonance imaging demonstrated a purely epidural lesion at the L1-L2 level without any bony involvement. Following an L1-L2 laminectomy for total excision of the lesion, the patient showed significant improvement. The histopathology was consistent with a pure capillary hemangioma.
Conclusion:The radiological presentation of purely epidural capillary hemangiomas are often similar to those of schwannomas and meningiomas. Surgical confirmation of the pathology, and gross total excision of these lesions is recommended.
Keywords: Epidural capillary hemangioma, meningiomas, schwannomas
INTRODUCTION
Capillary hemangiomas are very vascular malformations. Although 83% are located in the head or neck area,[
CASE HISTORY
A 50-year-old male presented with a 1-year history of low back pain and rapid 1-month onset of a severe paraparesis without bladder and bowel involvement.
Examinations
On examination, he exhibited proximal iliopsoas/quadriceps weakness at the 2/5 level while extensor hallucis longus (EHL) was 0/5 on the right and 1/5 on the left. He exhibited loss of patellar and Achilles responses, as well as decreased sensation to pin appreciation/vibration below the L1/L2 level. Laboratory examinations were within normal limits.
The magnetic resonance (MR) scan showed an isointense lesion 49 × 37 × 13 mm extending from the T12-L2 Level [




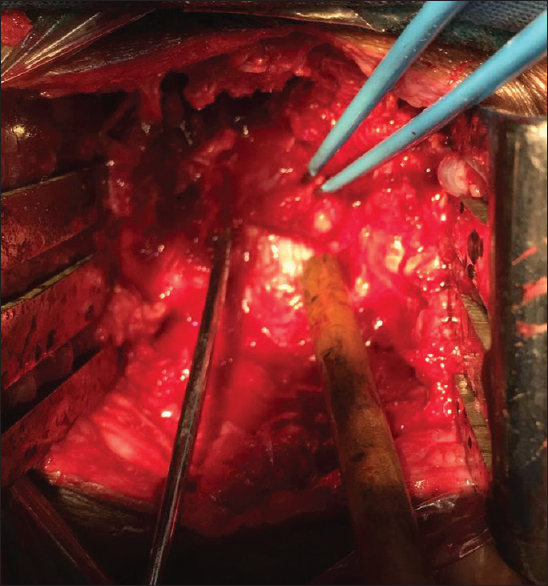
Surgery
Following an L1-L2 laminectomy, a 4 × 1 cm epidural, grayish, firm vascular lesion was observed filling the canal and extending through the right L1-L2 neural foramen. The lesion was easily dissected away from the dura and total excision of the mass was achieved [

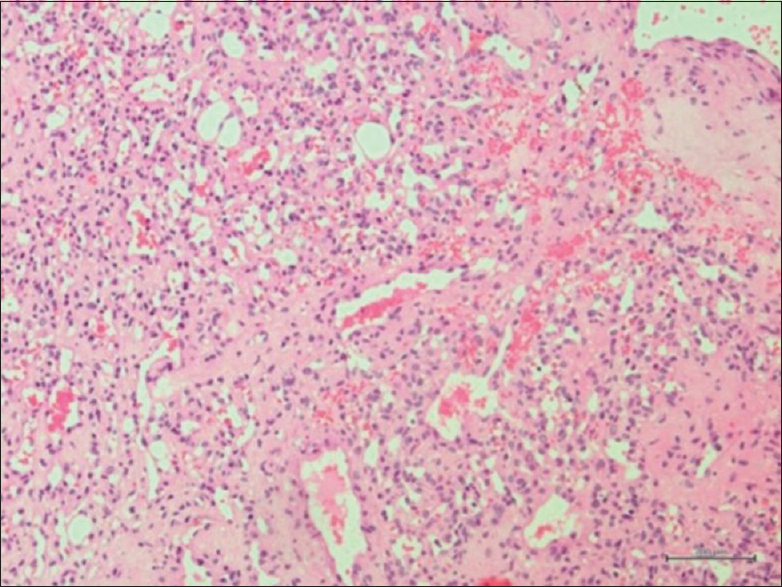
Histopathology
The lesion was vascular, composed of variable caliber blood vessels predominantly thin-walled and back to back. There were areas of hemorrhage and some vessels were thrombosed. The neoplasm was also poorly circumscribed [
DISCUSSION
Hemangiomas are congenital vascular malformations that pathologists frequently consider to be hamartomatous malformations. They are classified by the predominant type of vascular channel (capillary, cavernous, arteriovenous, or venous) observed on histologic examination. These are usually located in the soft tissue or bone but are mainly found in the spinal column.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alakandy LM, Hercules S, Balamurali G, Reid H, Herwadkar A, Holland JP. Thoracic intradural extramedullary capillary haemangioma. Br J Neurosurg. 2006. 20: 235-8
2. Aoyagi N, Kojima K, Kasai H. Review of spinal epidural cavernous hemangioma. Neurol Med Chir (Tokyo). 2003. 43: 471-5; discussion 476
3. Badinand B, Morel C, Kopp N, Tran Min VA, Cotton F. Dumbbell shaped epidural capillary hemangioma. AJNR Am J Neuroradiol. 2003. 24: 190-2
4. Bozkus H, Tanriverdi T, Kizilkiliç O, Türeci E, Oz B, Hanci M. Capillary hemangiomas of the spinal cord: Report of two cases. Minim Invasive Neurosurg. 2003. 46: 41-6
5. Caruso G, Galarza M, Borghesi I, Pozzati E, Vitale M. Acute presentation of spinal epidural cavernous angiomas: Case report. Neurosurgery. 2007. 60: E575-6; discussion E576
6. Gupta S, Kumar S, Banerji D, Pandey R, Gujral R. Magnetic resonance imaging features of an epidural spinal haemangioma. Australas Radiol. 1996. 40: 342-4
7. Hasan A, Guiot MC, Torres C, Marcoux J. A case of a spinal epidural capillary hemangioma: Case report. Neurosurgery. 2011. 68: E850-3

