

- Department of Neurosurgery, Nara Medical University, Nara Prefecture, Japan.
- Department of Radiology, Nara Medical University, Nara Prefecture, Japan.
Correspondence Address:
Ichiro Nakagawa
Department of Neurosurgery, Nara Medical University, Nara Prefecture, Japan.
DOI:10.25259/SNI-293-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ryosuke Maeoka, Ichiro Nakagawa, Koji Omoto, Takeshi Wada, Kimihiko Kichikawa, Hiroyuki Nakase. Stent-assisted coil embolization of unruptured vertebral artery dissecting aneurysms with the low-profile visualized intraluminal support stent, with five techniques: Technical note and case report. 19-Jun-2019;10:105
How to cite this URL: Ryosuke Maeoka, Ichiro Nakagawa, Koji Omoto, Takeshi Wada, Kimihiko Kichikawa, Hiroyuki Nakase. Stent-assisted coil embolization of unruptured vertebral artery dissecting aneurysms with the low-profile visualized intraluminal support stent, with five techniques: Technical note and case report. 19-Jun-2019;10:105. Available from: http://surgicalneurologyint.com/surgicalint-articles/9379/
Date of Submission
11-May-2019
Date of Acceptance
16-May-2019
Date of Web Publication
19-Jun-2019
Abstract
Background: Intracranial vertebral artery dissecting aneurysm (VADA) is rare and shows high morbidity and mortality rates when the aneurysm ruptures. Endovascular treatment for VADA is one of the optimal treatments, but the dominant side VA and its branches or perforators need to be preserved. We report a novel and successful stent-assisted coil embolization technique using the low-profile visualized intraluminal support (LVIS) stent, with five technical notes in three consecutive cases of unruptured vertebral artery dissecting aneurysm (VADA).
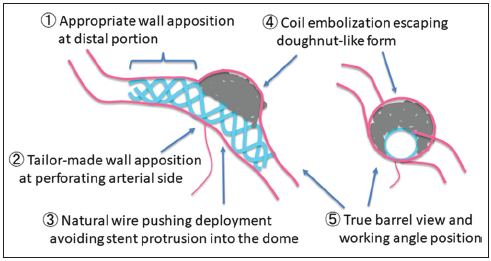
Case Description: We report three consecutive cases of unruptured VADA which involved a posterior inferior cerebellar artery (PICA), an anterior spinal artery, and perforators. Stent-assisted coil embolization with the LVIS stent was performed in all patients. The stent was carefully placed to obtain parent artery wall apposition at distal portion and with moderate pushing at aneurysm portion. The LVIS stent was placed with tailor-made wall apposition at perforating arterial side in the barrel view, and coil embolization was performed avoiding doughnut-like stent form to prevent perforator infarcts. All cases showed complete occlusion of the aneurysms with preservation of both parent artery and its branches and perforators patency. In three cases, clinical presentations were improved without ischemic complications. The median follow-up period was 1 year. At present, no recurrence and no complication have been observed.
Conclusion: We demonstrate the coil embolization of VADA using LVIS stent with five techniques. Our techniques for the treatment of VADA using LVIS stent are safe and can minimize ischemic complications by creating suitable wall apposition to the orifices of branches or perforators.
Keywords: Intracranial vertebral artery dissecting aneurysm, Ischemic complications, Low-profile visualized intraluminal support stent, Stent-assisted coil embolization
INTRODUCTION
Intracranial vertebral artery dissecting aneurysm (VADA) has been known as a cause of subarachnoid hemorrhage and infarcts of the posterior circulation. Various surgical techniques have been reported for the treatment of these lesions, but endovascular treatment could be one of the optimal treatments, obviating the need for complex skull base approaches. Endovascular treatment modalities include reconstructive techniques using stents with or without coil embolization and deconstructive techniques such as proximal occlusion or internal trapping.[
We report our technical tips of the low-profile visualized intraluminal support (LVIS) stent-assited coil embolization for intracranial VADA.
MATERIALS AND METHODS
We report three consecutive cases of unruptured VADA which involved a PICA, an ASA, and perforators. Stent-assisted coil embolization with the LVIS stent was performed in all patients. All procedures were performed at Nara Medical University. Informed consent was obtained from all patients included in this study. Information relating to the patients was collected from their medical record.
All procedures were performed under general anesthesia. All patients were pretreated with dual antiplatelet therapy (100 mg/day of aspirin and 75 mg/day of clopidogrel) for at least 7 days before the procedure. During the procedure, heparin was intravenously infused with the goal of achieving an activated clotting time of >250 s. Dual antiplatelet therapy was continued for 3 months after the procedure.
RESULTS
Case 1
A 59-year-old man suffered from the right Wallenberg syndrome due to the right VA dissection. Magnetic resonance angiography (MRA) showed a left unruptured VADA located on the dominant side. Follow-up MRA demonstrated that the VADA was getting bigger and stent-assisted coil embolization was planned for the preservation of the parent circulation. 3D rotational angiography (3DRA) revealed no remarkable perforating arteries involved in the VADA [
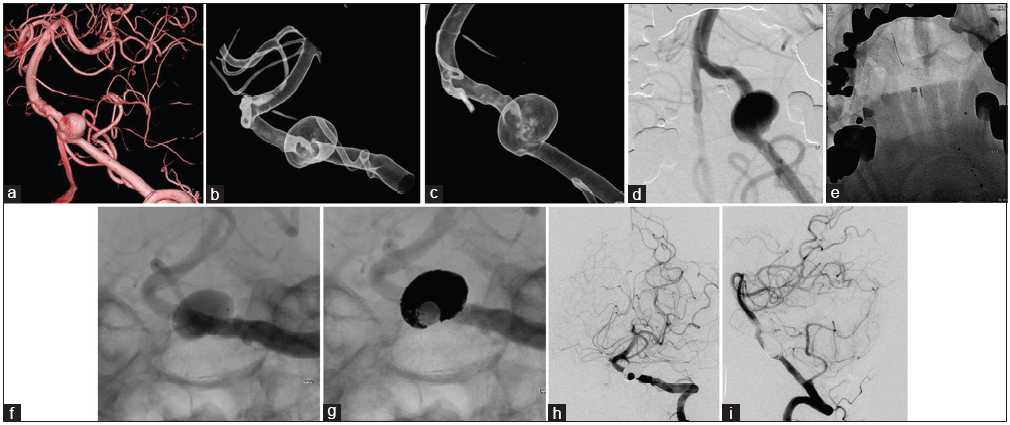
Figure 1
(a) 3D rotational angiography and digital subtraction angiography demonstrated a left vertebral artery dissecting aneurysm (10×13 mm in diameter). On 3D rotational angiography, a left vertebral artery dissecting aneurysm is located on the dominant side with no involvement of perforating arteries. (b) A 3D translucent road map view of the true barrel viewed position (B) and of the working position (C). (c) A 3D translucent road map view of the true barrel viewed position (B) and of the working position (C). (d and e) Deployment of the LVIS stent with “natural wire pushing.” (f and g) The LVIS stent was placed with “tailor-made wall apposition at perforating arterial side” and coil embolization with “escaping doughnut-like form” in the true barrel viewed position. (h and i) Digital subtraction angiography after 3 months shows complete occlusion and maintenance of the parent circulation.
Case 2
A 52-year-old man presented with headache and MRA showed a left unruptured VADA. He was introduced to our institute after enlargement of the aneurysm. DSA revealed a VADA on the dominant side with involvement of the orifice of the ASA [
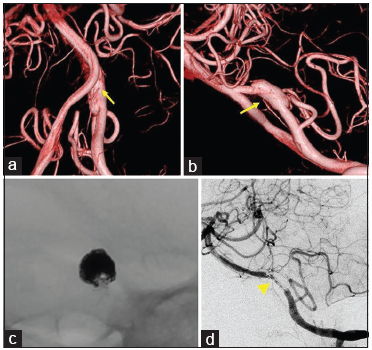
Figure 2
(a and b) 3D rotational angiography and digital subtraction angiography demonstrated a left vertebral artery dissecting aneurysm (5.6×5.2 mm in diameter). On 3D rotational angiography, a left vertebral artery dissecting aneurysm located on the dominant side with involving the orifice of anterior spinal artery (arrow). (c) The LVIS stent was placed with “tailor-made wall apposition at perforating arterial side.” Coil embolization was performed with “escaping doughnut-like form” in the true barrel viewed position. (d) Digital subtraction angiography after 3 months shows complete occlusion and maintenance of parent artery and anterior spinal artery circulation (arrowhead).
Case 3
A 66-year-old man showed enlarged left VADA involving the orifice of the PICA [
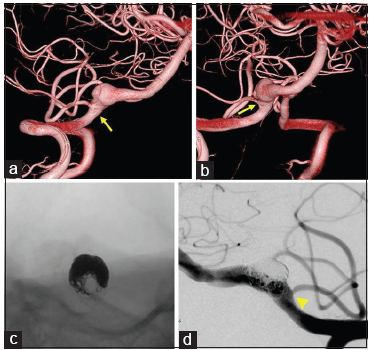
Figure 3
(a and b) 3D rotational angiography and digital subtraction angiography demonstrated a right vertebral artery dissecting aneurysm (9.1×8.4 mm in diameter). On 3D rotational angiography, a right vertebral artery dissecting aneurysm located on the dominant side with involving the orifice of the posterior inferior cerebellar artery (arrow). (c) The LVIS stent was placed with “tailor-made wall apposition at perforating arterial side.” Coil embolization was performed with “escaping doughnut-like form” in the true barrel viewed position. (d) Angiogram in the working position. Posterior inferior cerebellar artery patency is maintained (arrowhead).
DISCUSSION
Standard endovascular treatment for VADA had been proximal occlusion or internal trapping of the VA, but occlusion of the dominant VA parent artery could result in ischemic complications or hemodynamic alterations, risking contralateral VADA.[
However, some limitations of our techniques should be noted. First, it is difficult to treat when the perforator is on the aneurysm wall. There is no feasible way to protect the orifice of the perforator. Second, due to the low porosity of the LVIS stent, it is difficult to treat the recurrence of the aneurysms with trans-cell approach. Third, we report only three cases, the small number of cases in a single institution, and the short-term follow-up period. It is very scant to prove the efficacy of these techniques.
Many studies have reported the LVIS stent as safe and effective in the treatment of ruptured and unruptured intracranial saccular aneurysms.[
CONCLUSION
We report a novel stent-assisted coil embolization technique using the LVIS stent, with five techniques in three consecutive cases of unruptured VADA. These five techniques may minimize ischemic complications by creating suitable wall apposition to the orifices of branches or perforators. Our small case series demonstrates the coil embolization with LVIS stent with five techniques is safe and good clinical outcomes and suggests that it could improve the outcomes of endovascular treatment of the VADA.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Grossberg JA, Hanel RA, Dabus G, Keigher K, Haussen DC, Sauvageau E. Treatment of wide-necked aneurysms with the low-profile visualized intraluminal support (LVIS jr) device: A multicenter experience. J Neurointerv Surg. 2017. 9: 1098-102
2. Iosif C, Piotin M, Saleme S, Barreau X, Sedat J, Chau Y. Safety and effectiveness of the low profile visualized intraluminal support (LVIS and LVIS jr) devices in the endovascular treatment of intracranial aneurysms: Results of the TRAIL multicenter observational study. J Neurointerv Surg. 2018. 10: 675-81
3. Kühn AL, Kan P, Massari F, Lozano JD, Hou SY, Howk M. Endovascular reconstruction of unruptured intradural vertebral artery dissecting aneurysms with the pipeline embolization device. J Neurointerv Surg. 2016. 8: 1048-51
4. Natarajan SK, Lin N, Sonig A, Rai AT, Carpenter JS, Levy EI. The safety of pipeline flow diversion in fusiform vertebrobasilar aneurysms: A consecutive case series with longer-term follow-up from a single US center. J Neurosurg. 2016. 125: 111-9
5. Poncyljusz W, Biliński P, Safranow K, Baron J, Zbroszczyk M, Jaworski M. The LVIS/LVIS jr. Stents in the treatment of wide-neck intracranial aneurysms: Multicentre registry. J Neurointerv Surg. 2015. 7: 524-9
6. Shankar JJ, Quateen A, Weill A, Tampieri D, Cortes MD, Fahed R. Canadian registry of LVIS jr for treatment of intracranial aneurysms (CaRLA). J Neurointerv Surg. 2017. 9: 849-53
7. Siddiqui AH, Abla AA, Kan P, Dumont TM, Jahshan S, Britz GW. Panacea or problem: Flow diverters in the treatment of symptomatic large or giant fusiform vertebrobasilar aneurysms. J Neurosurg. 2012. 116: 1258-66
8. Sönmez Ö, Brinjikji W, Murad MH, Lanzino G. Deconstructive and reconstructive techniques in treatment of vertebrobasilar dissecting aneurysms: A systematic review and meta-analysis. AJNR Am J Neuroradiol. 2015. 36: 1293-8
9. van Rooij WJ, Sluzewski M. Perforator infarction after placement of a pipeline flow-diverting stent for an unruptured A1 aneurysm. AJNR Am J Neuroradiol. 2010. 31: E43-4
10. Zhang X, Zhong J, Gao H, Xu F, Bambakidis NC. Endovascular treatment of intracranial aneurysms with the LVIS device: A systematic review. J Neurointerv Surg. 2017. 9: 553-7

