

- Southern Tohoku Institute for Neuroscience, Koriyama City, Fukushima Prefecture, Japan
Correspondence Address:
Maddala Sundeep
Southern Tohoku Institute for Neuroscience, Koriyama City, Fukushima Prefecture, Japan
DOI:10.4103/sni.sni_102_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Maddala Sundeep, Yoshitaka Hirano, Susumu Iketani, Akiyoshi Konno. Surgical management of symptomatic ossified anterior longitudinal ligament: A case report. 13-Jun-2017;8:108
How to cite this URL: Maddala Sundeep, Yoshitaka Hirano, Susumu Iketani, Akiyoshi Konno. Surgical management of symptomatic ossified anterior longitudinal ligament: A case report. 13-Jun-2017;8:108. Available from: http://surgicalneurologyint.com/surgicalint-articles/surgical-management-of-symptomatic-ossified-anterior-longitudinal-ligament-a-case-report/
Date of Submission
11-Mar-2017
Date of Acceptance
05-Apr-2017
Date of Web Publication
13-Jun-2017
Abstract
Background:Ossified anterior longitudinal ligament (OALL) of the cervical spine can cause dysphagia, dyspnoea, and dysphonia, although these symptoms are rare.
Case Description:A 71-year-old male presented with gradually progressive dysphagia secondary to OALL. He underwent fiber optic endoscopy and lateral video fluoroscopy. The OALL extended from C4 to C7 and contributed to significant compression of the pharynx as demonstrated on plain cervical radiography, magnetic resonance (MR) imaging, and computed tomography (CT). Following microsurgical resection of the OALL, his symptoms improved.
Conclusions:This study focuses on the clinical and radiographic presentation of OALL; the latter utilizing plain X-rays, MR, and CT studies. Notably, surgical resection is straightforward and allows for immediate decompression of the pharynx as long as it is truly the symptomatic problem.
Keywords: Dysphagia, microsurgical resection, ossified anterior longitudinal ligament
INTRODUCTION
Symptomatic Ossified Anterior Longitudinal Ligament (OALL) of the cervical spine is rare, although common in men in their sixth or seventh decades of life.[
CASE DESCRIPTION
A 71-year-old male presented with dysphagia over a one year period. He initially underwent fiber optic endoscopy that revealed an anterior mass in the midline projecting into the middle pharynx [

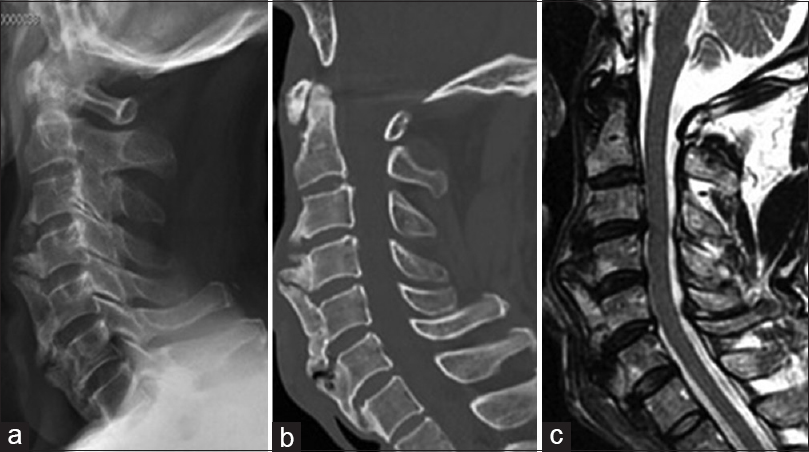
Figure 2
The preoperative lateral plain radiograph reveals beak like ossified anterior longitudinal ligament (OALL) projecting anteriorly at C4–5 (a), which is confirmed on mid-sagittal computed tomography (CT) image (b). The magnetic resonance T2 weighted image (c) shows minimal compression of the thecal sac at C3–4 disc level

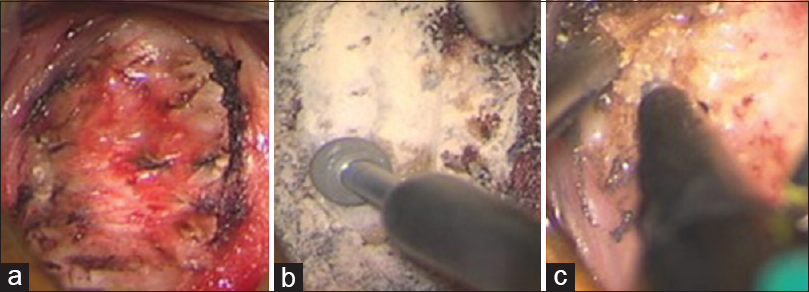
With increasing symptoms (e.g., frequent cough/hoarseness), the patient was reassessed the next year for surgery. There was difficulty during intubation due to the severe beak-like deformity and it was performed using enhanced direct video larygoscopy (McGRATH MAC, Medtronics, USA). A microscopic anterior cervical approach was utilized for removal of the OALL. It was largely removed with a bone rongeur and then smoothed using a high-speed drill [Figure
DISCUSSION
Dysphagia, dyspnoea, and dysphonia are common symptoms caused by OALL. Dysphagia secondary to OALL can be secondary to mechanical obstruction as well as chronic inflammation and fibrosis leading to dysfunction in peristalsis. McCafferty et al. stated that less than 10% of patients with dysphagia require surgical management. Plain radiography and CT images are helpful in identifying and distinguishing OALL from DISH and degenerative cervical osteophytes.[
LVF complemented with fiber optic endoscopy will contribute significantly to rule out other causes of oro-pharyngeal dysphagia such as malignancy, neurological impairment, diverticula, pharyngeal or oesophageal stenosis.[
Early surgery in symptomatic patients, particularly those with mechanical obstruction aids in the prevention of chronic inflammation and local fibrosis, which may otherwise cause delayed response. We have performed a microsurgical resection of the OALL using rongeurs, diamond drills, and the ultrasonic bone curette.
Surgical management in symptomatic OALL will prevent secondary complications of dysphagia, and improve the quality of life.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chen Y-R, Sung K, Tharin S. Symptomatic Anterior Cervical Osteophyte causing Dysphagia: Case Report, Imaging, and Review of the Literature. Cureus. 2016. 8: 473-
2. Epstein NE, Hollingsworth R. Ossification of the cervical anterior longitudinal ligament contributing to dysphagia. Case Report. J Neurosurg. 1999. 90: 261-3
3. Fattori B, Giusti P, Mancini V, Grosso M, Barillari MR, Bastiani L. Comparison between videofluoroscopy, fiberoptic endoscopy and scintigraphy for diagnosis of oro-pharyngeal dysphagia. Acta Otorhinolaryngol Ital. 2016. 36: 395-402
4. Hwang JS, Chough CK, Joo WI. Giant anterior cervical osteophyte leading to Dysphagia. Korean J Spine. 2013. 10: 200-2
5. Lecerf P, Malard O. How to diagnose and treat symptomatic anterior cervical osteophytes?. Eur Ann Otorhinolaryngol Head Neck Dis. 2010. 127: 111-6
6. Mizuno J, Nakagawa H, Song J. Symptomatic ossification of the anterior longitudinal ligament with stenosis of the cervical spine: A report of seven cases. J Bone Joint Surg Br. 2005. 87: 1375-9
7. Song J, Mizuno J, Nakagawa H. Clinical and radiological analysis of ossification of the anterior longitudinal ligament causing dysphagia and hoarseness. Neurosurgery. 2006. 58: 913-9

