

- Department of Neurosurgery, Baylor College of Medicine, Houston, Texas, USA
- Department of Radiology, University of Massachusetts Medical School, Worcester, Massachusetts, USA
Correspondence Address:
Peter Kan
Department of Neurosurgery, Baylor College of Medicine, Houston, Texas, USA
DOI:10.4103/2152-7806.157797
Copyright: © 2015 Kan P. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Kan P, Wakhloo AK, Mokin M, Puri A. Techniques in distal access of wide-necked giant intracranial aneurysms during treatment with flow diversion. Surg Neurol Int 28-May-2015;6:
How to cite this URL: Kan P, Wakhloo AK, Mokin M, Puri A. Techniques in distal access of wide-necked giant intracranial aneurysms during treatment with flow diversion. Surg Neurol Int 28-May-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/techniques-distal-access-wide%e2%80%91necked-giant-intracranial/
Abstract
Background:Accessing the normal distal vessel in treatment of wide-necked giant intracranial aneurysms with flow diversion can be difficult.
Case Description:Through illustrative cases, the authors present several useful techniques in distal access of wide-necked giant aneurysms during flow diversion treatment. Obtaining an optimal projection that separates the outflow limb from the aneurysm is most critical. Each of the three techniques described enabled the distal access to giant intracranial aneurysms during treatment with flow diversion.
Conclusion:The looped-around technique, balloon-assisted technique, and retrograde access are valuable strategies in crossing the aneurysm if direct distal access cannot be obtained.
Keywords: Distal access, flow diversion, giant intracranial aneurysms, neurovascular, wide-necked
With approval from the U.S. Food and Drug Administration of the Pipeline Embolization Device (PED), the use of flow diversion has become more common for the treatment of unruptured giant aneurysms in the anterior circulation that cannot be treated by traditional endovascular methods. Early results have been very encouraging, with occlusion rates of large and giant aneurysms approaching 90% at 6 months;[
FLOW DIVERSION PROCEDURE
All patients were treated with dual antiplatelets consisting of 325 mg of aspirin daily and 75 mg of clopidogrel daily for 5 days prior to the procedure. The degree of P2Y12 inhibition and aspirin response was tested with VerifyNow (Accumetrics, San Diego, CA) on the day of treatment. An aspirin response unit value of ≤550 and a Plavix Response Unit of ≤230 were considered to indicate an appropriate level of platelet inhibition for treatment. All procedures were performed under general anesthesia. Systemic heparin was used to achieve an activated clotting time of ≥250 s. To ensure robust proximal support, a triaxial system was used through femoral access in each case. This consisted of a 6 French shuttle sheath (Cook Medical, Bloomington, IN) placed in the common carotid artery prior to the bifurcation, a 5 French Navien distal access catheter (Covidien Vascular Therapies, Mansfield, MA) placed proximal to the neck of the aneurysm, and the delivery microcatheter for the flow diverter.
Case 1
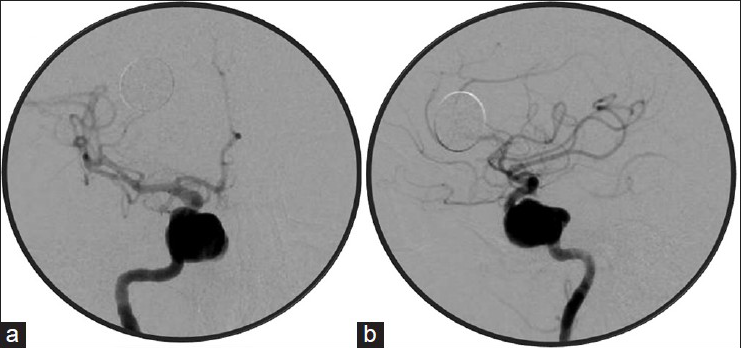
A 73-year-old female presented with an enlarging, giant right cavernous internal carotid artery (ICA) aneurysm [

Case 2
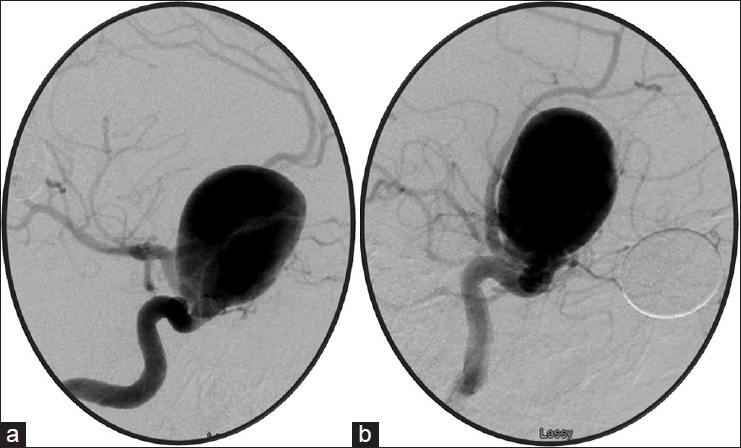
A 53-year-old female presented with a 1-week loss of visual acuity over her left eye. Catheter angiography demonstrated a giant left carotid ophthalmic aneurysm [


Case 3
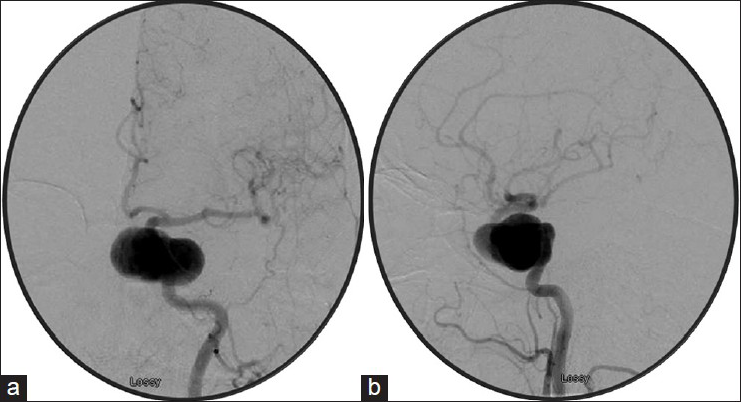
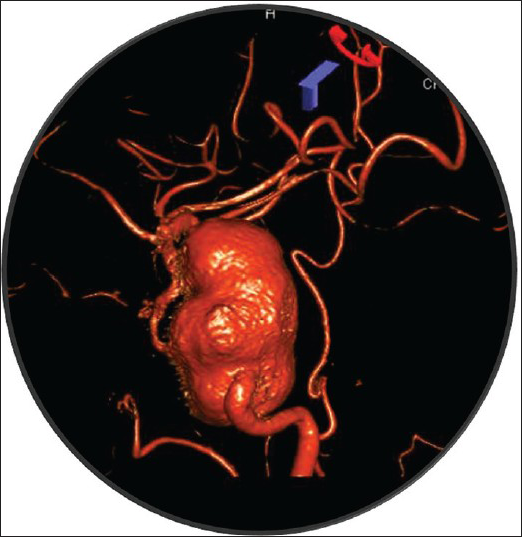
A 58-year-old female presented with headache. A computed tomography (CT) scan did not reveal subarachnoid hemorrhage. Magnetic resonance imaging (MRI) and subsequently catheter angiography demonstrated a 3 × 2-cm giant left cavernous ICA aneurysm [
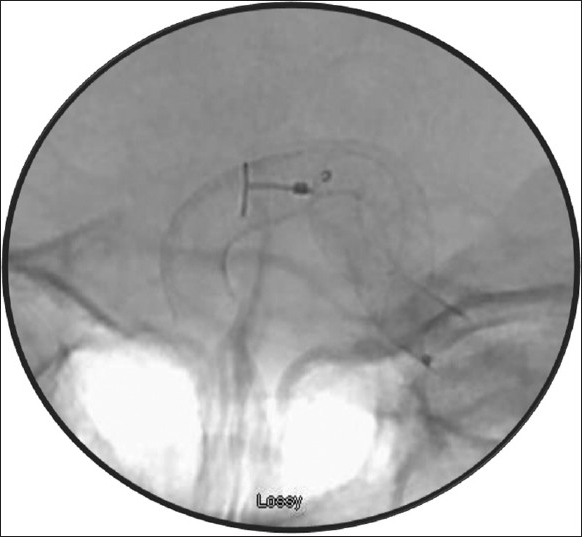
On a separate intervention, bilateral femoral groin access was obtained. A 5 French guide was placed in the right cervical ICA. An SL-10 microcatheter and a Synchro standard 014 wire were used to access the aneurysm retrograde across the anterior communicating artery [

DISCUSSION
The use of flow diverting stents has become more common for treatment of unruptured sidewall large and giant intracranial aneurysms in the anterior circulation that cannot be treated by traditional endovascular methods. Unlike intrasaccular coil embolization, its successful deployment relies on access to the normal vasculature distal to the aneurysm neck, which can be very challenging for the neurointerventionalist because the proximal and distal limbs of these aneurysms are often distant from each other with no intervening normal vessel. We highlight several techniques that facilitate the distal access of giant intracranial aneurysms during treatment with flow diversion.
The first and foremost step is to obtain a projection that separates the aneurysm from the outflow limb such that the outflow vessel can be clearly visualized. The optimal projection is best obtained from the three-dimensional rotational image on the workstation. In cases of giant aneurysms, there is often a delay in opacification of the outflow vessel because of the transit time of contrast in the aneurysm. As a result, we typically increase the delay before acquisition during three-dimensional rotational angiography to ensure that the outflow vessel is well visualized [
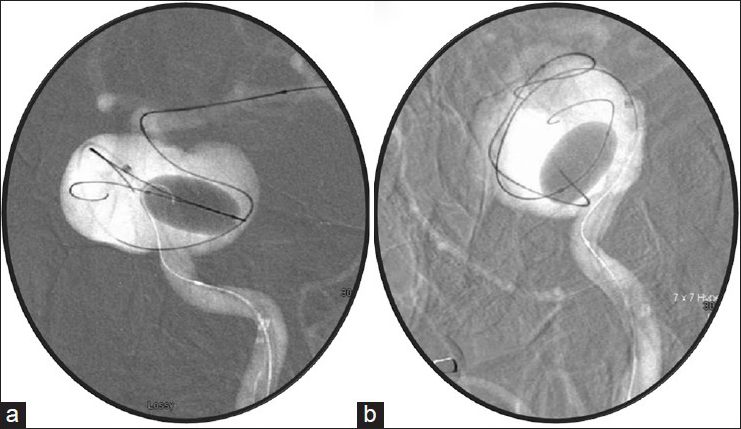
If the looped-around technique fails to engage the outflow limb as in case 3, a large balloon can be used to reduce the volume of the aneurysm to increase the chance of obtaining distal access. In this case, a larger distal access catheter (Navien 072) is required to allow simultaneous balloon and microcatheter placement into the aneurysm. Again, a trackable microcatheter is used to cross the now-smaller aneurysm with the above-mentioned looped-around technique. Once distal access is obtained, the balloon can then be removed. The catheter can then be reduced for device deployment.
Finally, if the above techniques were unsuccessful and the patient has an adequate anterior or posterior communicating artery, retrograde access of the aneurysm can be performed. A large snare can be used to capture the retrograde microwire into the microcatheter, which, in turn, can bring the microcatheter into the distal limb (“flossing”). At this point, anterograde access of the MCA can be obtained.
Flow diversion is emerging as an important technique in the armamentarium for treatment of unruptured large and giant intracranial aneurysms in the carotid circulation. Its successful deployment relies on access to the vasculature distal to the aneurysm neck. We have found that the above-mentioned techniques are valuable and practical to increase the success of flow diversion in the treatment of these difficult intracranial aneurysms.
References
1. Becske T, Kallmes DF, Saatci I, McDougall CG, Szikora I, Lanzino G. Pipeline for uncoilable or failed aneurysms: Results from a multicenter clinical trial. Radiology. 2013. 267: 858-68
2. Edwards L, Kota G, Morris PP. The sea anchor technique: A novel method to aid in stent-assisted embolization of giant cerebral aneurysms. J Neurointerv Surg. 2013. 5: e39-
3. Fargen KM, Velat GJ, Lawson MF, Hoh BL, Mocco J. The stent anchor technique for distal access through a large or giant aneurysm. J Neurointerv Surg. 2013. 5: e24-
4. Hauck EF, Natarajan SK, Langer DJ, Hopkins LN, Siddiqui AH, Levy EI. Retrograde trans-posterior communicating artery snare-assisted rescue of lost access to a foreshortened pipeline embolization device: Complication management. Neurosurgery. 2010. 67: S495-502
5. Snyder KV, Natarajan SK, Hauck EF, Mocco J, Siddiqui AH, Hopkins LN. The balloon anchor technique: A novel technique for distal access through a giant aneurysm. J Neurointerv Surg. 2010. 2: 363-7

