

- Department of Neurological Surgery, University of California, Sacramento, California, USA
- The Spine Surgery Institute, Cedars Sinai Medical Center, Los Angeles, California, USA
Correspondence Address:
Jared D. Ament
Department of Neurological Surgery, University of California, Sacramento, California, USA
The Spine Surgery Institute, Cedars Sinai Medical Center, Los Angeles, California, USA
DOI:10.4103/sni.sni_441_17
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Jared D. Ament, Tejas Karnati, Edwin Kulubya, Kee D. Kim, J. Patrick Johnson. Treatment of cervical radiculopathy: A review of the evolution and economics. 14-Feb-2018;9:35
How to cite this URL: Jared D. Ament, Tejas Karnati, Edwin Kulubya, Kee D. Kim, J. Patrick Johnson. Treatment of cervical radiculopathy: A review of the evolution and economics. 14-Feb-2018;9:35. Available from: http://surgicalneurologyint.com/surgicalint-articles/treatment-of-cervical-radiculopathy-a-review-of-the-evolution-and-economics/
Date of Submission
25-Nov-2017
Date of Acceptance
06-Dec-2017
Date of Web Publication
14-Feb-2018
Abstract
Background:The surgical treatment of cervical radiculopathy has centered around anterior cervical discectomy and fusion (ACDF). Alternatively, the posterior cervical laminoforaminotomy/microdiscectomy (PCF/PCM), which results in comparable outcomes and is more cost-effective, has been underutilized.
Methods:Here, we compared the direct/indirect costs, reoperation rates, and outcome for ACDF and PCF vs. PCM using PubMed, Medline, and Embase databases.
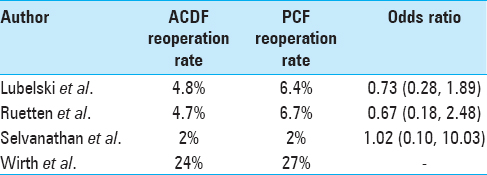
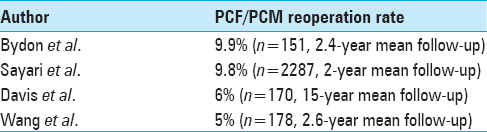
Results:There were no significant differences between the re-operative rates of PCF/PCM (2% to 9.8%) versus ACDF (2% to 8%). Direct costs of ACDF were also significantly higher; the 1-year cost-utility analysis demonstrated that ACDF had $131,951/QALY while PCM had $79,856/QALY.
Conclusion:PCF/PCM for radiculopathy are safe and more cost-effective vs. ACDF, and have similar clinical outcomes.
Keywords: Cervical degenerative disc disease, cervical disc herniation, cost-effectiveness, posterior approach, posterior cervical microdiscectomy, quality of life
INTRODUCTION
Although posterior cervical laminoforaminotomy/microdiscectomy (PCM/PCF) are only infrequently performed, studies have shown no significant difference in outcomes and suggested improved cost-effectiveness for these procedures vs. anterior cervical discectomy/fusion (ACDF).[
MATERIALS AND METHODS
Indications
The PCF/PCM procedure is highly effective in treating patients with cervical radiculopathy due to degenerative lateral/foraminal disease that affects the exiting nerve root.[
Benefits of open laminoforaminotomy for lateral/foraminal diskectomy/spur excision
The open cervical laminoforaminotomy offers excellent direct exposure of the foraminally exiting nerve root and full maneuverability with a down-biting curette/microdissectors for the excision of lateral/foraminal discs/spurs. Alternatively, although the mini-open microsurgical or tubular minimally invasive approach theoretically limits soft tissue manipulation, there is also more limited visualization and field of operative dissection, increasing the risk of retained foraminal disc/spur and/or neurological injury.
Technical points for mini-open laminoforaminotomy/microdiscectomy
After obtaining baseline somatosensory evoked (SEP), motor evoked potential (MEP), and electromyographic (EMG) potentials/monitoring, an awake nasotracheal fiberoptic or glide scope intubation (with appropriate local anesthetics) are performed. Using a local anesthetic, a Mayfield 3-pin head holder is applied and the patients are placed prone on bilateral chest rolls. Next, for an open procedure, the midline incision is followed by subperiosteal dissection carried out from the midline to the facet joint. For the tubular MIS, a paramedian incision (approximately 2 cm from the midline) may alternatively be utilized. (e.g., two-thirds covering the interlaminar space; one-third covering the facet joint). Performing an adequate medial facetectomy/foraminotomy, with shaved-down/angled Kerrison rongeurs, allows the excision of disc material and/or osteophytes using down-biting curettes and microdissectors. If these latter maneuvers are hampered by the limited exposure provided by the tubular MIS approach, conversion to an open procedure for better visualization/maneuverability is essential to avoid neural/other injuries.
Reoperation rates
Although some studies document higher revision rates for PCF/PCM vs. ACDF, most show similar outcomes for both groups.[
Cost-effectiveness
Although data vary, PCF/PCM often appear more cost-effective compared to ACDF. In a study by Mansfield et al., the direct costs of ACDF were 89–182% greater vs. PCF/PCM.[
CONCLUSION
In the cervical spine, PCM/PCF offers a safer and more cost-effective lateral/foraminal nerve root decompression without the need for fusion as with ACDF. Unfortunately, we have entire generations of spine surgeons who are relatively uncomfortable with the PCF/PCM procedure, and, it is essential to recover this “lost art.”
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alvin MD, Lubelski D, Abdullah KG, Whitmore RG, Benzel EC, Mroz TE. Cost utility analysis of anterior cervical discectomy and fusion with plating (ACDFP) versus posterior cervical Foraminotomy (PCF) for patients with single-level cervical radiculopathy at 1-year follow-up. Clin Spine Surg. 2016. 29: E67-72
2. Henderson CM, Hennessy RG, Shuey HM Jr, Shackelford EG. Posterior- lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery. 1983. 13: 504-12
3. Herkowitz HN, Kurz LT, Overholt DP. Surgical management of cervical soft disc herniation. A comparison between the anterior and posterior approach. Spine. 1990. 15: 1026-30
4. Liu WJ, Hu L, Chou PH, Wang JW, Kan WS. Comparison of Anterior Cervical Discectomy and Fusion versus Posterior Cervical Foraminotomy in the Treatment of Cervical Radiculopathy: A Systematic Review. Orthop Surg. 2016. 8: 425-31
5. Lubelski D, Healy AT, Silverstein MP, Abdullah KG, Thompson NR, Riew KD. Reoperation rates after anterior cervical discectomy and fusion versus posterior cervical foraminotomy: A propensity-matched analysis. Spine J. 2015. 15: 1277-83
6. Mansfield HE, Canar WJ, Gerard CS, O’Toole JE. Single-level anterior cervical discectomy and fusion versus minimally invasive posterior cervical foraminotomy for patients with cervical radiculopathy: A cost analysis. Neurosurg Focus. 2014. 37: E9-
7. Sayari AJ, Tuchman A, Cohen JR, Hsieh PC, Buser Z, Wang JC. Risk and Cost of Reoperation After Single-Level Posterior Cervical Foraminotomy: A Large Database Study. Global Spine J. 2017. 7: 116-22
8. Tumialan LM, Ponton RP, Gluf WM. Management of unilateral cervical radiculopathy in the military: The cost effectiveness of posterior cervical foraminotomy compared with anterior cervical discectomy and fusion. Neurosurg Focus. 2010. 28: 1-6
9. Wang TY, Lubelski D, Abdullah KG, Steinmetz MP, Benzel EC, Mroz TE. Rates of anterior cervical discectomy and fusion after initial posterior cervical foraminotomy. Spine J. 2015. 15: 971-6
10. Wirth FP, Dowd GC, Sanders HF, Wirth C. Cervical discectomy. A prospective analysis of three operative techniques. Surg Neurol. 2000. 53: 340-346

