

- Department of Orthopaedics and Spine, Private Practice, Jaypee Hospital, Noida, Uttar Pradesh,
- Departments of Neurosurgery Nanoori Hospital, Seoul, Republic of Korea,
- Department of Ortho-Spine Surgery, Sir Ganga Ram Hospital, New Delhi, India,
- Department of Neurosurgery, University of Michigen, Michigen, United States,
- Departments of Orthopaedics, Nanoori Hospital, Seoul, Republic of Korea,
- Medical School, Medical School University of Debrecen, Debrecen, Hungary.
Correspondence Address:
Hyeun-Sung Kim
Departments of Neurosurgery Nanoori Hospital, Seoul, Republic of Korea,
DOI:10.25259/SNI_173_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ravindra Singh, Hyeun-Sung Kim, Nitin Adsul, Osama Nezar Kashlan, Sung Woon Oh, Jung Hoon Noh, Soeng Cheol Moon, Chang Hwan Park, Il Tae Jang, Seong Hoon Oh. X-rays and scans can fail to differentiate hip pathology from lumbar spinal stenosis: Two case reports. 23-Aug-2019;10:165
How to cite this URL: Ravindra Singh, Hyeun-Sung Kim, Nitin Adsul, Osama Nezar Kashlan, Sung Woon Oh, Jung Hoon Noh, Soeng Cheol Moon, Chang Hwan Park, Il Tae Jang, Seong Hoon Oh. X-rays and scans can fail to differentiate hip pathology from lumbar spinal stenosis: Two case reports. 23-Aug-2019;10:165. Available from: http://surgicalneurologyint.com/surgicalint-articles/9592/
Date of Submission
05-Mar-2019
Date of Acceptance
26-Jun-2019
Date of Web Publication
23-Aug-2019
Abstract
Background: Occasionally, hip pathologies may present alone or combined with lumbar spine pathology, especially lumbar stenosis. Although the history and clinical examination may help differentiate between the two, hip X-rays alone without accompanying magnetic resonance imaging (MRI) studies may prove unreliable.
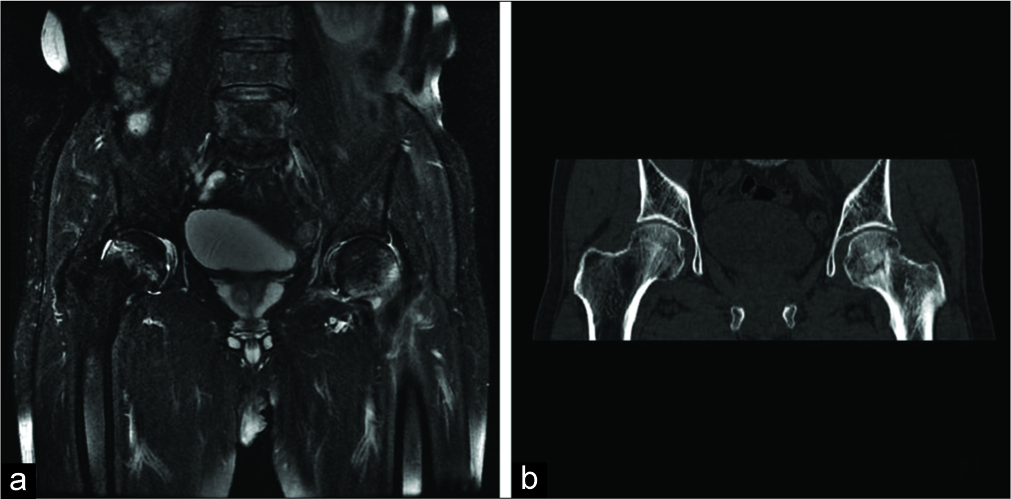
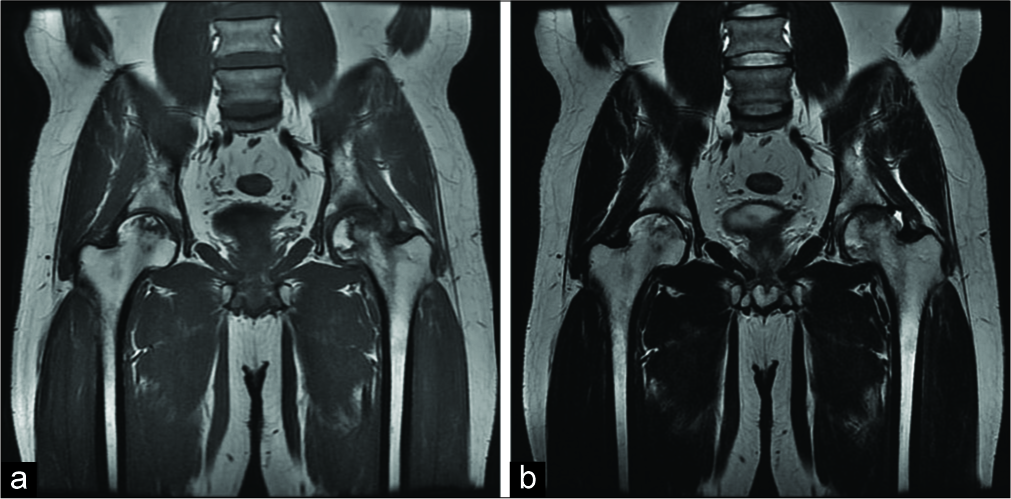
Case Descriptions: Case 1 – A 72-year-old male presented with the sudden onset of severe back and left posterior thigh pain. Straight leg raising test was positive at 70° (right) and 60° (left), and he had left lower extremity numbness and weakness. The lumbar MRI showed L5-S1 spinal stenosis. Although X-rays of both hips were negative, the MRI showed bilateral femoral neck fractures. He underwent screw fixation of the hip fractures and later underwent endoscopic decompression of the spinal stenosis. Case 2 – A 35-year-old male presented with low backache and right hip pain of 1 month’s duration. The neurological examination was normal, except for positive straight leg raising bilaterally at 60°. The spine MRI was normal. However, despite negative X-ray of both hips, the hip MRI revealed avascular necrosis (AVN) of both femoral heads requiring subsequent orthopedic management.
Conclusion: Hip pathology may mimic lumbar spinal stenosis. In the two cases presented, plain X-rays failed to document hip fractures (case 1) and AVN (case 2), respectively, both of which were later diagnosed on MRI studies.
Keywords: Avascular necrosis, Backache, Femoral head, Fracture, Hip, Neck of femur, Spinal stenosis, Spine
INTRODUCTION
Some patients with what appears to be lumbar spinal stenosis, with/without positive magnetic resonance imaging (MRI) studies, may have hip disease. However, hip X-rays alone may fail in certain circumstances, to document hip significant pathology. Here, we present two such cases, in which bilateral femoral head fractures (case 1) and avascular necrosis (AVN) (case 2) were missed on X-rays alone but ultimately diagnosed on MRI examinations.
CASE REPORTS
Case 1
A 72-year-old male presented with the sudden onset of severe back (visual analog scale [VAS] 10) and the left posterior thigh pain (VAS score 7) following a fall 2 months ago. Straight leg raising test was positive on the right at 70º and 60º on the left; findings also included a partial left foot drop (dorsiflexion 3/5) with L5 hyperesthesias. The lumbar MR showed L5-S1 stenosis [


Case 2
A 35-year-old male patient presented with low backache and right hip pain (VAS 7) of 1 month’s duration following an insignificant traumatic event. Straight leg raising test was positive at 60° bilaterally, but the neurological examination was normal. Both spine X-rays and the lumbar MRI were normal. X-rays of both hips were negative, but the MRI of studies showed Ficat Stage I of AVN of both femoral heads [

DISCUSSION
Differentiation between hip and spine pathology may sometimes be difficult.[
Hip disease “missed” on X-rays alone but diagnosed with MR
As demonstrated in the two cases presented, X-rays alone may have “missed” hip pathology. In both cases, hip fractures and AVN were diagnosed on MRI scans.[
CONCLUSION
Hip disease can mimic spinal stenosis. In certain cases, hip X-rays may be negative, but hip MR scans may be warranted to document other significant hip pathology as in these two cases involving bilateral hip fractures and AVN, respectively.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Baker AD, Banaszkiewicz P, Kader D.editors. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. Classic Papers in Orthopaedics. London: Springer; 2014. p.
2. Braly BA, Beall DP, Martin HD. Clinical examination of the athletic hip. Clin Sports Med. 2006. 25: 199-210
3. Ficat RP. Idiopathic bone necrosis of the femoral head. Early diagnosis and treatment. J Bone Joint Surg Br. 1985. 67: 3-9
4. Pathak G, Parker MJ, Pryor GA. Delayed diagnosis of femoral neck fractures. Injury. 1997. 28: 299-301
5. Sandhu HS. Management of fracture neck of femur. Indian J Orthop. 2005. 39: 130-6
6. Sembrano JN, Polly DW Jr. How often is low back pain not coming from the back?. Spine (Phila Pa 1976). 2009. 34: E27-32
7. Steinberg ME, Hayken GD, Steinberg DR. A quantitative system for staging avascular necrosis. J Bone Joint Surg Br. 1995. 77: 34-41
8. Steinmet MP, Benzel EC.editorsBenzel’s Spine Surgery. Philadelphia, PA: Elsevier; 2018. p. 624-830
9. Wen DY, Propeck T, Singh A. Femoral neck stress injury with negative bone scan. J Am Board Fam Pract. 2003. 16: 170-4

