

- National Brain Aneurysm Center at the John Nasseff Neuroscience Institute, Allina Health, Twin Cities, MN, USA
Correspondence Address:
Eric S. Nussbaum
National Brain Aneurysm Center at the John Nasseff Neuroscience Institute, Allina Health, Twin Cities, MN, USA
DOI:10.4103/2152-7806.165202
Copyright: © 2015 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nussbaum ES, Lowary J, Nussbaum LA. A multidisciplinary approach to the treatment of severe cerebral vasospasm following bacterial meningitis: A case report and literature review. Surg Neurol Int 14-Sep-2015;6:148
How to cite this URL: Nussbaum ES, Lowary J, Nussbaum LA. A multidisciplinary approach to the treatment of severe cerebral vasospasm following bacterial meningitis: A case report and literature review. Surg Neurol Int 14-Sep-2015;6:148. Available from: http://surgicalneurologyint.com/surgicalint_articles/a-multidisciplinary-approach-to-the-treatment-of-severe-cerebral/
Abstract
Background:Although cerebrovascular complications of bacterial meningitis are common, postmeningitic cerebral vasospasm significant enough to result in ischemic injury has been reported in only limited fashion.
Case Description:We describe a case of severe cerebral vasospasm following streptococcal meningitis managed successfully with emergency suboccipital decompression, extracranial-intracranial bypass, intra-arterial vasodilator infusion, and maximal medical therapy. To our knowledge, this may be the first case in which surgical cerebral revascularization has been utilized to limit ischemic injury in the setting of postmeningitic cerebral vasospasm.
Conclusions:Patients presenting with abrupt neurological decline following recent treatment for bacterial meningitis may be suffering from a reversible vasoconstriction of the cerebral arteries, and prompt aggressive treatment can result in a favorable outcome even in patients who present in very poor neurological condition.
Keywords: Bypass, ischemia, meningitis, stroke, vasospasm
INTRODUCTION
Although cerebrovascular complications of bacterial meningitis are common, postmeningitic cerebral vasospasm significant enough to result in ischemic injury has been reported in only limited fashion.[
CASE DESCRIPTION
This 46-year-old cattle rancher presented with headaches, fevers, and sinusitis. A lumbar puncture revealed elevated white blood cell count, and gram-stain and cultures demonstrated Streptococcus viridans. The patient was started on intravenous antibiotic therapy and responded with prompt improvement. He was subsequently switched to an oral antibiotic regimen but returned to the hospital 2 weeks later with visual disturbance, worsening headache, and intermittent dysarthria. He experienced a rapid decline in level of consciousness necessitating endotracheal intubation and was then transferred to our facility for further care.
On arrival, the patient was deeply comatose. A magnetic resonance imaging (MRI) examination of the brain revealed bilateral posterior cerebral artery (PCA) territory ischemic changes with a sizeable right posterior inferior cerebellar artery (PICA) infarction [
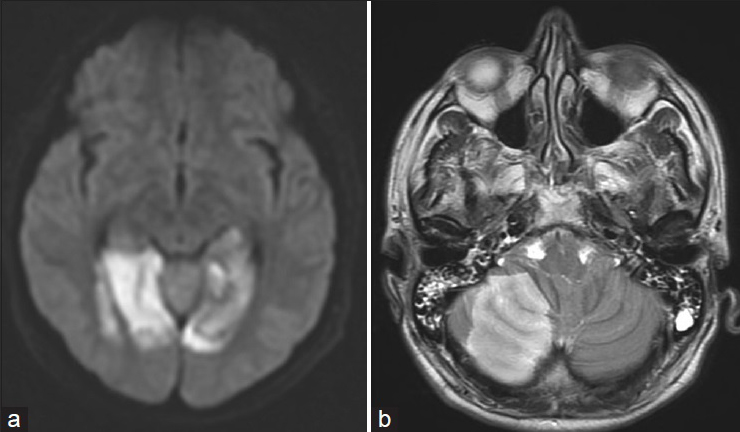
An emergency angiogram demonstrated severe spasm of the posterior circulation with the basilar artery having an almost thread-like appearance and moderate vasospasm of the anterior circulation [

Figure 2
(a) Right internal carotid arteriogram demonstrates moderate spasm of the A1 (arrow) and more severe narrowing of the A2 (arrowhead) segments of the anterior cerebral artery. (b) Vertebral arteriographic image shows severe narrowing of the distal vertebral arteries (arrowheads) with thread-like appearance (arrow) of the basilar artery itself
The patient was taken to the operating room where a right frontal ventriculostomy was performed revealing moderately elevated intracranial pressure. The patient then underwent a suboccipital craniectomy and duraplasty for posterior fossa decompression. An intrathecal microcatheter was left in place at the end of this procedure, advanced into the cerebellopontine angle cistern to reach the basilar artery. At this point, the occipital artery (OA) was dissected, and a small occipital supratentorial parasagittal craniotomy was performed through which the OA was anastomosed to a cortical branch of the PCA with 11–0 interrupted suture [

The patient was maintained in barbiturate coma for 5 days with daily angiographic examinations demonstrating persistent severe spasm of the cerebral arteries which were repeatedly treated with intra-arterial verapamil infusion. Intrathecal papaverine infusions through the surgically placed microcatheter were performed on a daily basis as well. Repeated angiographic examinations demonstrated slow improvement in the degree of arterial narrowing and filling of the posterior cerebral territory through the bypass [

After 2 weeks, the patient began to regain consciousness; and by the 3rd week, he was clearly following simple commands. The ventriculostomy was discontinued, and the patient was subsequently transferred to an inpatient rehabilitation facility. He was maintained on antibiotic therapy for 3 months, prednisone for 6 weeks, and aspirin indefinitely. Six months later, the patient had made a striking recovery with only limited visual field impairment and was back to work on a near full-time basis [

DISCUSSSION
Cerebrovascular complications have been described in 15–20% of adults with community-acquired bacterial meningitis.[
Several studies have shown that transcranial Doppler ultrasound evaluation of patients with acute bacterial meningitis reveals elevated velocities suggesting some degree of vascular narrowing in a surprisingly significant percentage of patients studied, but reversible vascoconstriction severe enough to result in ischemic injury is quite unusual.[
Recently, a number of investigators have described the use of endovascular therapies to manage patients with cerebral vasospasm resulting from infectious meningitis.[
In our case, the severe narrowing of the basilar artery and its branches likely resulted in the patients’ rapid neurological decline and associated areas of ischemic change on MRI. Once the patient developed edema related to his PICA infarction, it became evident a decompressive procedure was required to prevent a fatal herniation syndrome, and with the patient already in the operating room, a decision was made to attempt to augment intracranial flow in the posterior circulation with a bypass procedure. It is impossible to know for sure whether the patient would have recovered as well without the bypass. We suspect that the maximally aggressive multidisciplinary approach to optimize cerebral blood flow including optimization of cardiac output and the cerebral microenvironment by the neurocritical care team, the use of intra-arterial vasodilator therapy by our interventional neuroradiology colleagues, and the use of bypass combined with intrathecal infusion of papaverine likely all contributed to the ultimately favorable outcome.
Finally, it should be noted that narrowing and irregularity of the cerebral arteries in the setting of infectious meningitis have been variably described as vasospasm, vasculitis, and vasculopathy.[
CONCLUSIONS
We report an unusual case of particularly severe cerebral vasospasm following bacterial meningitis. This may be the first such case managed in part with surgical cerebral revascularization as one aspect of therapy. Patients presenting with abrupt neurological decline following recent treatment for bacterial meningitis may be suffering from a reversible vasoconstriction of the cerebral arteries, and prompt aggressive treatment can result in a favorable outcome even in patients who present in very poor neurological condition.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors wish to thank Bridget Ho, CCRC with the John Nasseff Neuroscience Institute Research Department for her assistance with manuscript preparation and with references.
Commentary
- Editor in Chief.
jia@surgicalneurologyint.com
This is an outstanding paper with many lessons for the reader and neurosurgeons. First, the patient presented with widespread vasospasm and infarction. A very creative, skilled, and talented neurosurgeon who was willing to break convention and aggressively treat this patient performed a suboccipital craniotomy to relieve the swelling in the posterior fossa, and at the same time did an occipital to posterior cerebral artery territory bypass to provide blood to the posterior circulation that was compromised. Over time, the bypass increased as the vasospasm relented and provided perfusion to the vascular territory. The patient was placed in barbiturate coma in the interval, a technique that has its own complications. What is also dramatic is the disappearance 6 months later of the “infarcts” as shown by diffusion-weighted imaging (DWI) on magnetic resonance, which few would believe. Hence, the DWI changes were not indicative of infarction but ischemia. This is a seminal paper on a new approach to cerebral vasospasm in multiple modality treatments by an aggressive, creative, innovative neurosurgeon.
Many years ago, I had a case of extreme meningitis that was not responsive to antibiotics. From work I had done in the laboratory using hypothermic cerebral ventricular perfusion to isolate various parts of the brain, I thought that this idea might apply to my patient. Hence, I placed a ventricular catheter and a lumbar catheter and perfused ringer's solution through the ventricles and the cerebrospinal fluid. I do not think that the patient made it. You could not use antibiotics at the time as penicillin was known to produce seizures. I have often thought that someone ought to do a laboratory experiment in this same manner, with antibiotics to see if these extreme cases of meningitis can be resolved.
References
1. Batjer H, Samson D. Use of extracranial-intracranial bypass in the management of symptomatic vasospasm. Neurosurgery. 1986. 19: 235-46
2. Buechner D, Gelfand MS, Cleveland KO. Percutaneous transluminal angioplasty in a patient with vasospasm due to staphylococcal meningitis. J Neurosurg. 2012. 117: 103-6
3. Chaichana K, Riley LH, Tamargo RJ. Delayed cerebral vasospasm secondary to bacterial meningitis after lumbosacral spinal surgery: Case report. Neurosurgery. 2007. 60: E206-7
4. DiNubile MJ, Boom WH, Southwick FS. Septic cortical thrombophlebitis. J Infect Dis. 1990. 161: 1216-20
5. Ferris EJ, Rudikoff JC, Shapiro JH. Cerebral angiography of bacterial infection. Radiology. 1968. 90: 727-34
6. Haring HP, Rötzer HK, Reindl H, Berek K, Kampfl A, Pfausler B. Time course of cerebral blood flow velocity in central nervous system infections. A transcranial Doppler sonography study. Arch Neurol. 1993. 50: 98-101
7. Hu YC, Newman CB, Bristol R, McDougall CG, Albuquerque FC. Percutaneous transluminal angioplasty in a patient with vasospasm secondary to coccidioidal meningitis: Case report and review of the literature. J Neurointerv Surg. 2011. 3: 62-5
8. Igarashi M, Gilmartin RC, Gerald B, Wilburn F, Jabbour JT. Cerebral arteritis and bacterial meningitis. Arch Neurol. 1984. 41: 531-5
9. Kastenbauer S, Pfister HW. Pneumococcal meningitis in adults: Spectrum of complications and prognostic factors in a series of 87 cases. Brain. 2003. 126: 1015-25
10. Klein M, Koedel U, Pfefferkorn T, Zeller G, Woehrl B, Pfister HW. Arterial cerebrovascular complications in 94 adults with acute bacterial meningitis. Crit Care. 2011. 15: R281-
11. Komotar RJ, Zacharia BE, Valhora R, Mocco J, Connolly ES. Advances in vasospasm treatment and prevention. J Neurol Sci. 2007. 261: 134-42
12. Pfister HW, Borasio GD, Dirnagl U, Bauer M, Einhäupl KM. Cerebrovascular complications of bacterial meningitis in adults. Neurology. 1992. 42: 1497-504
13. Pugin D, Copin JC, Goodyear MC, Landis T, Gasche Y. Persisting vasculitis after pneumococcal meningitis. Neurocrit Care. 2006. 4: 237-40
14. Ries S, Schminke U, Fassbender K, Daffertshofer M, Steinke W, Hennerici M. Cerebrovascular involvement in the acute phase of bacterial meningitis. J Neurol. 1997. 244: 51-5
15. Taqui A, Koffman L, Hui F, Gomes J, Hussain MS, Bain M. Intra-arterial vasodilator therapy for parainfectious cerebral vasospasm. J Neurol Sci. 2014. 340: 225-9
16. van de Beek D, de Gans J, Tunkel AR, Wijdicks EF. Community-acquired bacterial meningitis in adults. N Engl J Med. 2006. 354: 44-53
17. Weststrate W, Hijdra A, de Gans J. Brain infarcts in adults with bacterial meningitis. Lancet. 1996. 347: 399-

