

- Department of Stem Cell Biology, School of Medicine, Konkuk University, Seoul, Korea
- Liebe Animal Medical Center, Seoul, Korea
- Department of Food Bioscience, College of Biomedical and Health Science, Konkuk University, Chung-ju, Korea
Correspondence Address:
C-Yoon Kim
Department of Food Bioscience, College of Biomedical and Health Science, Konkuk University, Chung-ju, Korea
DOI:10.4103/2152-7806.190476
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Kim C, Hwang I, Kim H, Jang S, Kim HS, Lee W. Accelerated recovery of sensorimotor function in a dog submitted to quasi-total transection of the cervical spinal cord and treated with PEG. Surg Neurol Int 13-Sep-2016;7:
How to cite this URL: Kim C, Hwang I, Kim H, Jang S, Kim HS, Lee W. Accelerated recovery of sensorimotor function in a dog submitted to quasi-total transection of the cervical spinal cord and treated with PEG. Surg Neurol Int 13-Sep-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/accelerated-recovery-sensorimotor-function-dog-submitted-quasi%e2%80%91total-transection-cervical-spinal-cord-treated-peg/
Abstract
Background:A case report on observing the recovery of sensory-motor function after cervical spinal cord transection.
Case Description:Laminectomy and transection of cervical spinal cord (C5) was performed on a male beagle weighing 3.5 kg. After applying polyethylene glycol (PEG) on the severed part, reconstruction of cervical spinal cord was confirmed by the restoration of sensorimotor function. Tetraplegia was observed immediately after operation, however, the dog showed stable respiration and survival without any complication. The dog showed fast recovery after 1 week, and recovered approximately 90% of normal sensorimotor function 3 weeks after the operation, although urinary disorder was still present. All recovery stages were recorded by video camera twice a week for behavioral analysis.
Conclusion:While current belief holds that functional recovery is impossible after a section greater than 50% at C5-6 in the canine model, this case study shows the possibility of cervical spinal cord reconstruction after near-total transection. Furthermore, this case study also confirms that PEG can truly expedite the recovery of sensorimotor function after cervical spinal cord sections in dogs.
Keywords: Cervical spinal cord transection, dog, polyethylene glycol, sensorimotor function
INTRODUCTION
It is a clinical dogma that there is no recovery from full transection of the spinal cord at whatever level as seen, for instance, after stab wounds.[
However, if the section is greater than 50% (of a hemisection), results are similar to a complete section. For example, in a patient, whose spinal cord was almost completely divided at C7/T1, only sensory disturbance was slightly improved at 4 months after the injury.[
The recently proposed GEMINI spinal cord fusion protocol[
In this paper, we report on a dog whose cervical spinal cord was transected >90% at visual inspection, and that showed motor recovery within 3 weeks of surgery. In patients with stab wounds to the spinal cord, there is no known method to refuse their severed cord and even in partial wounds, where recovery in many cases takes months to years.
The dog in this experiment was submitted to a sharp transection and treated with polyethylene glycol (PEG). PEG is a fusogen that has the capacity to restore the integrity of severed cell membranes[
CASE REPORT
The experiment was carried out in accordance with the guidelines of the animal ethics committees and approved by the Institutional Animal Care and Use Committee of the Konkuk University (Seoul, South Korea). A male Beagle (Orient Bio, Seongnam, Korea) dog weighing 3.5 kg at the time of surgery was included in the study. The dog was housed in a cage under simulated daylight conditions with alternating 12-hour light-dark cycles and had free access to food and water.
The dog was starved 12 hours prior to the operation to prepare for the paralysis of the digestive system post-operation. Anesthesia was first induced by propofol (10 mg/kg), and respiratory anesthesia (isofurane 2%) was maintained through a ventilator. Constant heart rate was maintained and monitored (electrocardiogram). After the surgical site was sterilized, an incision was made on the skin and the upper trapezius muscle in order to expose the spinous process of the 5th cervical vertebra (C5); the location was confirmed by C-arm fluoroscopy [
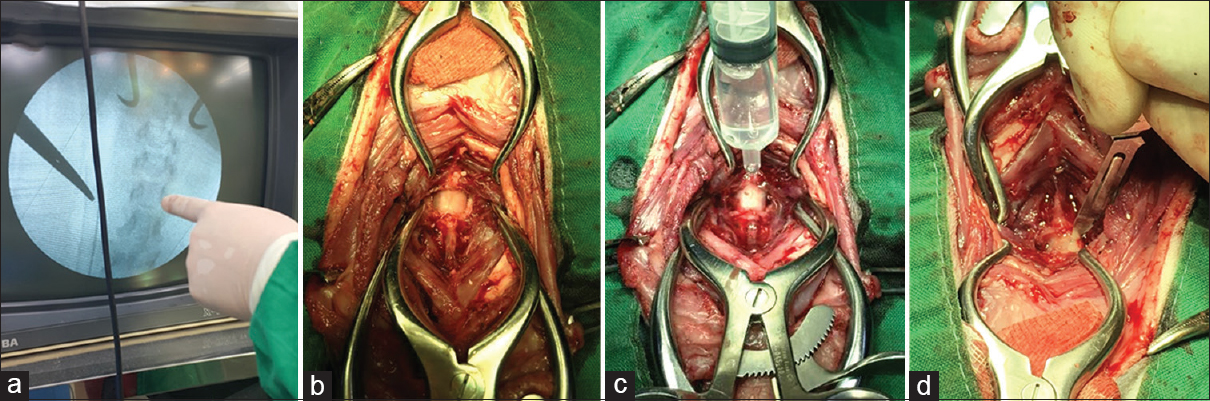
The dorsal part of C5 was removed with a bone rongeur, and the cervical cord was isolated [
Finally, the surgical site was prepared by applying PEG (PEG MW 400, Sigma-Aldrich, USA) until the cord was submerged [
After the transection, bleeding was controlled by applying surgifoam (Ethicon, USA), coagulated blood was suctioned out, and more PEG was added. Then, the dura mater was sutured by pulling 5 mm of each section so that the severed stumps were in contact. Coagulated blood was thoroughly removed, and additional PEG (5 ml) was applied before definitive dural closure. The surgical site was sutured by layer (muscle and then skin).
The dog was weaned from anesthesia. After voluntary respiration and consciousness were confirmed, the dog was taken to the intensive care unit (ICU) for 24 hours after the operation, and was treated with low doses of sedatives to minimize the stress from total paralysis. The dog was treated with antibiotics and sedatives for 1 week after the operation, and was supported by 5% dextrose and electrolyte solution (Halfsol, Daihan Pharm, Korea) and total parenteral nutrition.
Video files were recorded for analyzing functional recovery twice a week (Video), and behavioral functions were measured using the modified Frankel score (MFS)[
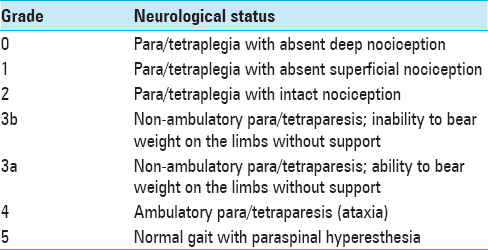
Twenty-four hours after the surgery, tetraplegia and absence of four-limb deep pain perception were observed; involuntary shaking of the limbs was observed at 48 hours. Restoration of respiratory control was confirmed by whining. The sound stopped intermittently when the dog was unable to control respiration, however, this had improved considerably after 48 hours to the extent that the dog could make sounds at will. Tetraplegia continued for 72 hours post-operation [

DISCUSSION
Results in the dog, although in need of confirmation in larger samples (in progress), are spectacular and, to the best of our knowledge, have never been reported in the literature. Sensory function was restored in parts of the animal's body in 48 hours, and small movement of the limbs were observed within a week. As reported, a section greater than 50% at C5-6 in the canine model leads to no recovery of respiration and death,[
No neurophysiologic testing was conducted and the animal was not sacrificed for histologic analysis; these tests were not part of the experimental protocol that focused on motor and sensory recovery following the use of fusogens. Similarly, there is no credible explanation for this recovery other than postulating that PEG acted according to the principles laid out in previous papers.[
If confirmed, these data open a new vista on the treatment of sectional spinal cord injury in man.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video is Availabe on: www.surgicalneurologyint.com
Acknowledgement
We thank Prof Canavero for assistance in writing the paper and assisting with the interpretation of the data.
References
1. . Stab wounds of the spinal cord. Br Med J. 1978. 1: 1093-4
2. Bitar Alatorre WE, Garcia Martinez D, Rosales Corral SA, Flores Soto ME, Velarde Silva G, Portilla de Buen E. Critical ischemia time in a model of spinal cord section. A study performed on dogs. Eur Spine J. 2007. 16: 563-72
3. Canavero S. HEAVEN: The head anastomosis venture Project outline for the first human head transplantation with spinal linkage (GEMINI). Surg Neurol Int. 2013. 4: S335-42
4. Canavero S, Ren X, Kim CY, Rosati E. Neurologic foundations of spinal cord fusion (GEMINI). Surgery. 2016. 160: 11-9
5. Cha YH, Cho TH, Suh JK. Traumatic cervical cord transection without facet dislocations--A proposal of combined hyperflexion-hyperextension mechanism: A case report. J Korean Med Sci. 2010. 25: 1247-50
6. Dlouhy BJ, Dahdaleh NS, Howard MA. Radiographic and intraoperative imaging of a hemisection of the spinal cord resulting in a pure Brown-Sequard syndrome: Case report and review of the literature. J Neurosurg Sci. 2013. 57: 81-6
7. Dran G, Fontaine D, Litrico S, Grellier P, Paquis P. Stabwound of the cervical spinal cord. Two case reports. Neurochirurgie. 2005. 51: 476-80
8. Griffin JFt, Levine J, Kerwin S. Canine thoracolumbar invertebral disk disease: Pathophysiology, neurologic examination, and emergency medical therapy. Compendium. 2009. 31: E2-
9. Kim CY. PEG-assisted reconstruction of the cervical spinal cord in rats: Effects on motor conduction at 1 h. Spinal Cord. 2016. p.
10. Lao LF, Zhong GB, Liu ZD. Transection of double-level spinal cord without radiographic abnormalities in an adult: A case report. Orthop Surg. 2013. 5: 302-4
11. Lee HM, Kim NH, Park CI. Spinal cord injury caused by a stab wound--A case report. Yonsei Med J. 1990. 31: 280-4
12. Lee SH, Chung YN, Kim YH, Kim YJ, Park JP, Kwon DK. Effects of human neural stem cell transplantation in canine spinal cord hemisection. Neurol Res. 2009. 31: 996-1002
13. Manzone P, Domenech V, Forlino D. Stab injury of the spinal cord surgically treated. J Spinal Disord. 2001. 14: 264-7
14. Richter-Turtur M, Krueger P, Wilker D, Angstwurm H. Cervical transverse spinal cord injury caused by knife stab injury. Der Unfallchirurg. 1990. 93: 4-5
15. Rubin G, Tallman D, Sagan L, Melgar M. An unusual stab wound of the cervical spinal cord: A case report. Spine. 2001. 26: 444-7
16. Shahlaie K, Chang DJ, Anderson JT. Nonmissile penetrating spinal injury. Case report and review of the literature. J Neurosurg Spine. 2006. 4: 400-8
17. Takahashi I, Iwasaki Y, Abumiya T, Imamura H, Houkin K, Saitoh H. Stab wounds of the spinal cord by a kitchen knife: Report of a case. No shinkei geka. 1991. 19: 255-8
18. Ye Y, Kim CY, Miao Q, Ren X. Fusogen-assisted rapid reconstitution of anatomophysiologic continuity of the transected spinal cord. Surgery. 2016. 160: 20-5

