

- WFNS Cerebrovascular Diseases and Therapy Committee, Tokyo, Toyoake, Japan
- Japan Neurosurgical Society, Tokyo, Toyoake, Japan
- Department of Neurosurgery, Fujita Health University School of Medicine, Toyoake, Japan
DOI:10.4103/2152-7806.187491
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sano H, Inamasu J, Kato Y, Satoh A, Murayama Y, . Modified world federation of neurosurgical societies subarachnoid hemorrhage grading system. Surg Neurol Int 01-Aug-2016;7:
How to cite this URL: Sano H, Inamasu J, Kato Y, Satoh A, Murayama Y, . Modified world federation of neurosurgical societies subarachnoid hemorrhage grading system. Surg Neurol Int 01-Aug-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/modified-world-federation-neurosurgical-societies-subarachnoid-hemorrhage-grading-system/
Sir,
The World Federation of Neurosurgical Societies (WFNS) scale for grading patients with aneurysmal subarachnoid hemorrhage (SAH) was originally published in 1988,[
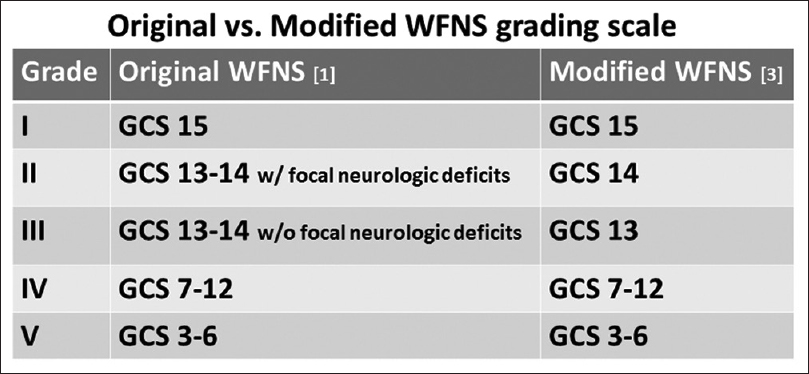
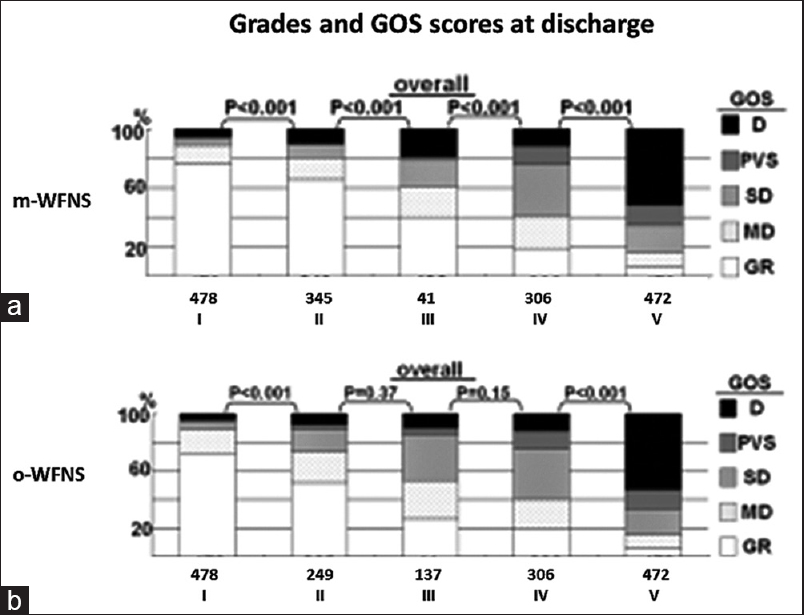
Figure 2
Mean GOS scores at discharge showing that in the m-WFNS scale, there was significant difference between any neighboring grades (a). By contrast, in the o-WFNS scale, the significant difference was observed only between grade I/II and between grade IV/V patients (b). Originally published as Figure 4 by Sano H et al.: Modified World Federation of Neurosurgical Societies subarachnoid hemorrhage grading system. World Neurosurg 2015;83:801-7. Permission granted from Elsevier Inc
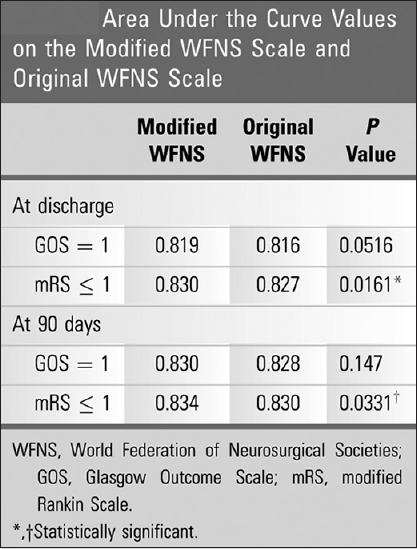
Figure 3
The results of receiver operating characteristic curve analysis showing that the m-WFNS scale had significantly higher area under the curve values (i.e. better outcome predictability) than the o-WFNS scale by mRS. Originally published as Table 2 by Sano H et al.: Modified World Federation of Neurosurgical Societies subarachnoid hemorrhage grading system. World Neurosurg 2015;83:801-7. Permission granted from Elsevier Inc
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The original article (same title) was published in World Neurosurgery (Volume 83, Issue 5, Pages 801–807, May 2015) Copyright for the reuse of Figures/Tables has been obtained from the publisher (Elsevier Inc.).
References
1. Drake CG. Report of World Federation of Neurological Surgeons Committee on a universal subarachnoid hemorrhage scale. J Neurosurg. 1988. 68: 985-6
2. Sano H, Satoh A, Murayama Y, Kato Y, Origasa H, Inamasu J. Modified World Federation of Neurosurgical Societies subarachnoid hemorrhage grading system. World Neurosurg. 2015. 83: 801-7
3. van Heuven AW, Dorhout Mees SM, Algra A, Rinkel GJ. Validation of a prognostic subarachnoid hemorrhage grading scale derived directly from the Glasgow Coma Scale. Stroke. 2008. 39: 1347-8

