

- Department of Neurosurgery, General Kamiiida Daiichi Hospital, Scientific Committee of Japanese Gamma Knife Society, Japan
- Department of Neurosurgery, Komaki City Hospital, Scientific Committee of Japanese Gamma Knife Society, Japan
- Department of Neurosurgery, Osaka General Medical Center, Scientific Committee of Japanese Gamma Knife Society, Japan
- Department of Neurosurgery, Yokohama Rosai Hospital, Scientific Committee of Japanese Gamma Knife Society, Japan
- Department of Neurosurgery, Rakusai Shimizu Hospital, Scientific Committee of Japanese Gamma Knife Society, Japan
- Department of Neurosurgery, Shinsuma General Hospital, Scientific Committee of Japanese Gamma Knife Society, Japan
- Department of Neurosurgery, Tokyo Women's Medical University, Scientific Committee of Japanese Gamma Knife Society, Japan
Correspondence Address:
Yoshihisa Kida
Department of Neurosurgery, Tokyo Women's Medical University, Scientific Committee of Japanese Gamma Knife Society, Japan
DOI:10.4103/2152-7806.157071
Copyright: © 2015 Kida Y. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Kida Y, Hasegawa T, Iwai Y, Shuto T, Satoh M, Kondoh T, Hayashi M. Radiosurgery for symptomatic cavernous malformations: A multi-institutional retrospective study in Japan. Surg Neurol Int 14-May-2015;6:
How to cite this URL: Kida Y, Hasegawa T, Iwai Y, Shuto T, Satoh M, Kondoh T, Hayashi M. Radiosurgery for symptomatic cavernous malformations: A multi-institutional retrospective study in Japan. Surg Neurol Int 14-May-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/radiosurgery-symptomatic-cavernous-malformations/
Abstract
Background:A group study for symptomatic cavernous malformation (CM) treated with gamma knife (GK) surgery was performed.
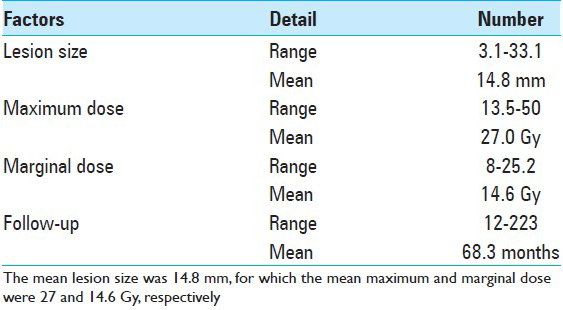
Methods:A total of 298 cases collected from 23 GK centers across Japan were included. Hemorrhage was the most common manifestation, followed by seizures and neurological deficits. Most of the lesions were located in the brainstem and basal ganglia, followed by the cerebral or cerebellar hemispheres. The CMs, which had a mean diameter of 14.8 mm, were treated using GK surgery with a mean marginal dose of 14.6 Gy.
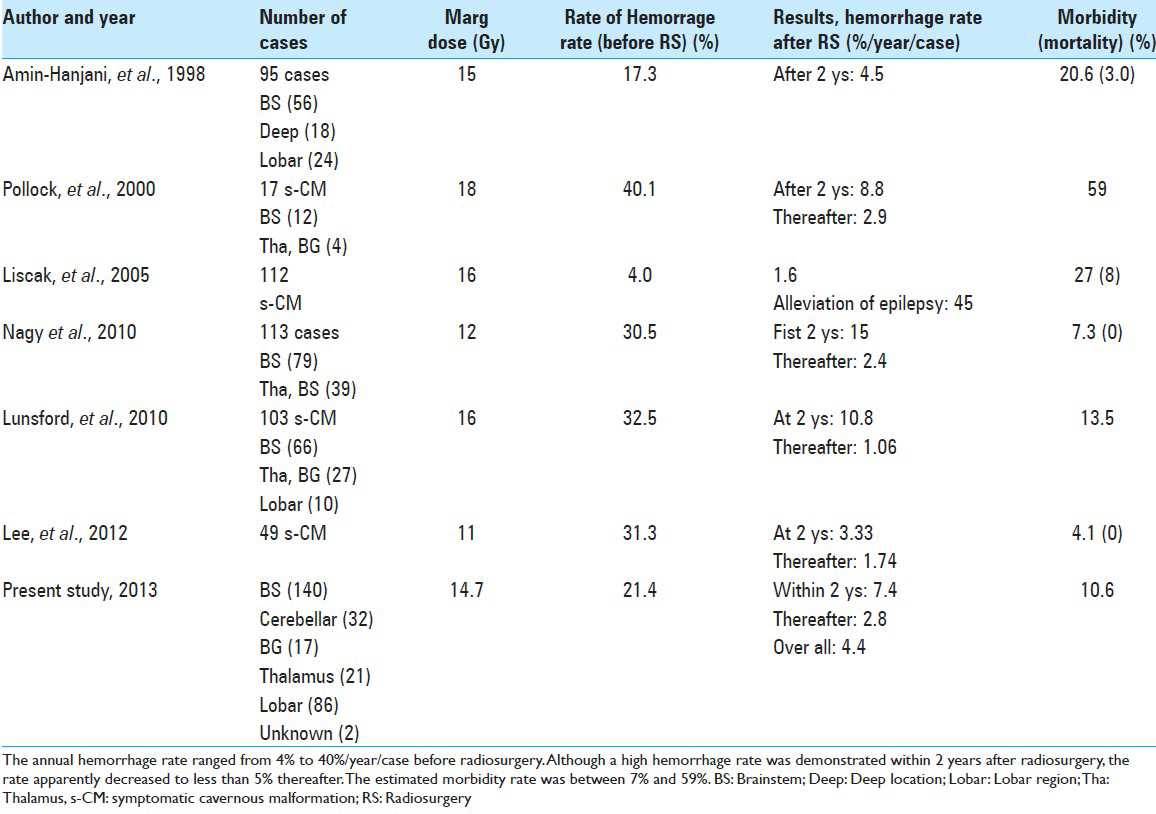
Results:In terms of hemorrhage-free survival (HFS), a marked dissociation was confirmed between the hemorrhage and seizure groups, while no obvious difference was noted between sexes. Superficial CMs located in cerebellum or lobar regions responded to the treatment better than deeply located CMs in the basal ganglia or brainstem. No significant difference of dose-dependent response was seen for three different ranges of marginal dose: Less than 15 Gy, between 15 and 20 Gy, and more than 20 Gy. Complications were more frequent after a marginal dose of over 15 Gy and in patients with lesions more than 15 mm in diameter. The rates of annual hemorrhage were estimated to be 7.4% during the first 2 years after radiosurgery and 2.8% thereafter. The overall hemorrhage rate after radiosurgery was 4.4%/year/patient.
Conclusion:The risk of hemorrhage is considerably reduced after GK treatment. The HFS as well as annual hemorrhage rate after GK treatment was apparently superior to that after conservative treatment for symptomatic CMs. To optimize the success of GK treatment, it is important to reduce the incidence of complications.
Keywords: Cavernous malformation, gamma knife, radiosurgery, symptomatic lesion, vascular anomaly
INTRODUCTION
Progress in neuroimaging has enabled cavernous malformations (CMs) in the brain to be easily detected using standard imaging studies, particularly magnetic resonance imaging (MRI). However, a differential diagnosis from thrombosed arteriovenous malformation (AVM), venous anomaly, or capillary hemangioectasia is not always easy. Thus the term “angiographically occult vascular malformation“ has been used in the medical literature. However, most of these lesions are believed to be CMs. A majority of CMs are clinically very silent and are often detected incidentally. Silent lesions should not be treated with surgery and should instead be managed conservatively using a so-called “wait-and-see” strategy. Some CM lesions, however, show very aggressive behaviors, with frequent bleeding, intractable seizures, or neurological deficits presenting during a short period of time.[
MATERIALS AND METHODS
Since the first installation of a gamma knife (GK) facility in Japan in 1990, 55 GK centers for radiosurgery have been established. Approximately half of these centers are currently performing GK treatment for symptomatic CMs (s-CMs). With the cooperation of the Scientific Committee of the Japanese Society of Gamma Knife, this multi-institutional retrospective study was planned and conducted with the permission of the Ethics Committee of the participating institutions.
In this study, a questionnaire was distributed and the following data were collected from each GK center in Japan. Data on the initial symptoms, location and size of the lesions, and treatment methods used at the time of the first episode were collected. Then, details regarding the radiosurgery procedure including the lesion site, lesion volume, and marginal dose of radiosurgery were investigated. Data on the subsequent occurrence of symptomatic episodes and the treatment used for such episodes as well as the final neurological status and outcome, along with the available imaging studies, were also requested.
GK treatment was performed at each of the participating institutions using a GK B, 4C, or Perfexion device (ELEKTA Instruments AB). The software used for dose planning was either KULA system or GammaPlan (ELEKTA Instruments AB). All the cases treated with GK were symptomatic, chiefly with hemorrhage, and epilepsy, neurological deficits in a few cases. No asymptomatic ones were included in this series. In general, whole lesions including the low-intensity rim were covered for supratentorial and cerebellar CMs, whereas only the core of the lesion was covered for lesions located in the brainstem or basal ganglia. After radiosurgery, follow-up studies using MRI were performed every 3 months during the first year and at least every 6 months thereafter. Finally, the radiological findings at the last follow-up were described in terms of complete remission (CR), partial remission (PR), minor response (MR), no change (NC) or progression (PG). Hemorrhage was defined as a new area of blood density on CT imaging in association with or without a neurological symptom or sign. New foci of high signal intensity on T1-weighted MR images, volume expansion of the lesions and edematous changes of surrounding brain were also carefully studied.
The final clinical status was classified into five categories as follows:
Excellent: No symptoms;
Good: Minimal or intermittent nondisabling symptoms;
Fair: Moderate disability, independent of others;
Poor: Major disability, dependent on others, progressive symptoms;
Dismal: Death, vegetative state.
Statistical analyses were performed using Fisher's exact two-tailed test for comparison of proportions by JMP-R 9.0.2 (2010, SAS Institute INC). For hemorrhage rates after diagnosis and treatment, survival analysis technique were used to compare Kaplan–Meier curves with log-rank test. Statistical significance was defined as P < 0.05. The annual hemorrhage rate (AHR) was defined as number of hemorrhages divided by total follow-up years.
RESULTS
Results of questionnaire and sample acquired
A total of 298 cases were collected from 23 GK centers located across Japan, including 23 GK institutions, consisting of 42% of all sites in Japan. They were treated with GK from 1991 to 2012, and with a sufficient follow-up period at least more than 12 months. The patient characteristics, such as their age and sex, the location of the lesion, and the mean lesion size, are listed in [
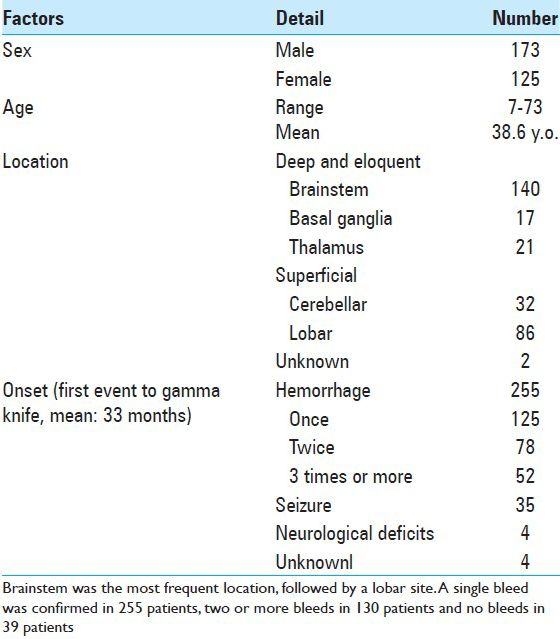
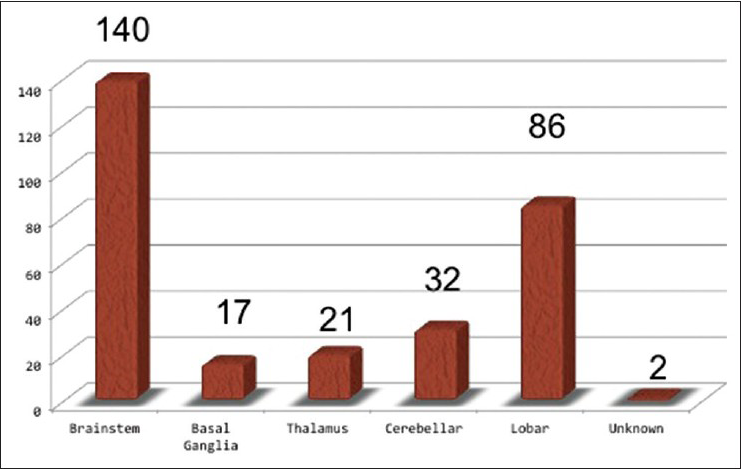
The majority of cases presented with hemorrhage (255 cases) prior to radiosurgery. Among them, a single hemorrhage occurred in 125 cases, two hemorrhages occurred in 78 cases, and three or more hemorrhages occurred in 52 cases. Thirty-five cases initially presented with seizure, and four cases presented with neurological deficits [
Radiosurgery with gamma knife in all centers
The lesion diameter at the time of radiosurgery ranged from 3.1 to 33.1 mm with a mean diameter of 14.8 mm. These lesions were treated using GK surgery with a mean marginal dose of 14.6 Gy [
Results after treatment
Radiological changes after radiosurgery
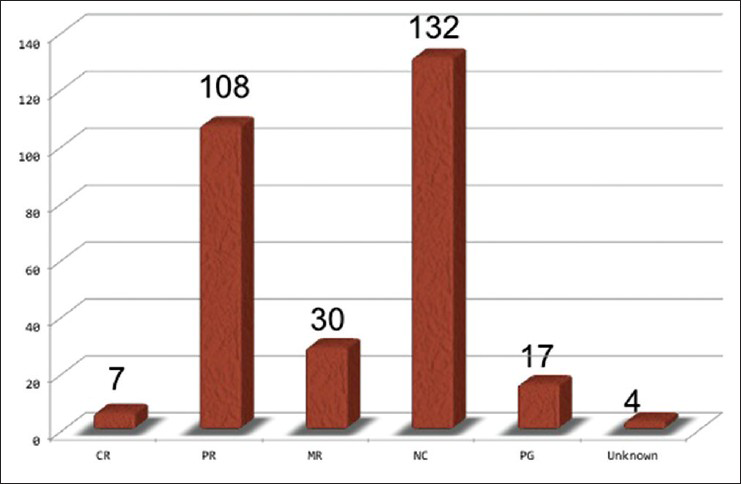
Almost half of the lesions showed some shrinkage, but the remaining lesions showed no change in size over a long time period. A few lesions increased in size mostly because of overt bleeding or minor hemorrhage after radiosurgery [
Hemorrhage-free survival
After radiosurgery, rebleeding or new bleeding occurred in 61 cases (18.3%). Regarding the onset patterns, further bleeding occurred in the cases that had initially presented with hemorrhage. The frequency of hemorrhage before radiosurgery, either single, two or more, did not significantly influence the hemorrhage-free survival (HFS) after radiosurgery (P = 0.1605) [
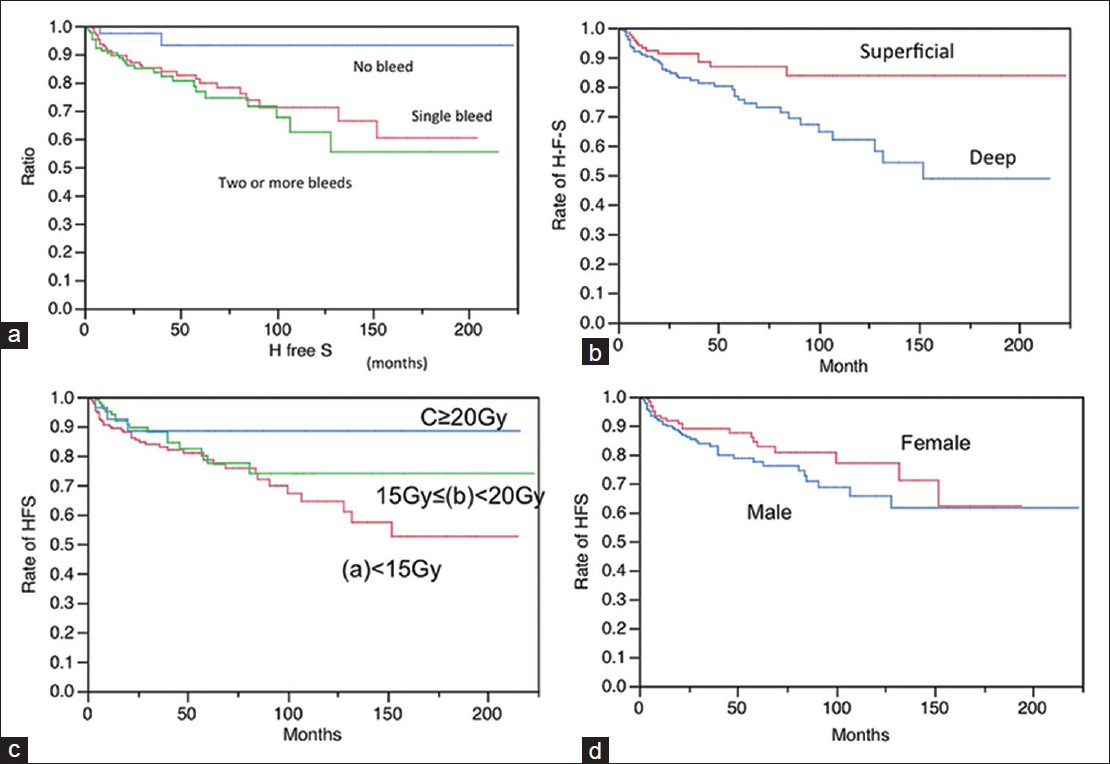
Figure 3
Hemorrhage-free survival (HFS) following radiosurgery according to various factors. (a) Onset, a: Single hemorrhage b: Two or more hemorrhages c: No hemorrhage (a vs b: Not significant, a vs c: Significant, b vs c: Significant) (b)Location the HFS was reasonably long in cases with superficial locations of the lesions, such as lobar and cerebellar lesions. In contrast, it was apparently worse in cases with deep locations of the lesions, such as the basal ganglia, thalamus, and brainstem. Superficial: Lobar, Cerebellar Deep: Brainstem, Basal ganglia, Thalamus (P =0.0077) (d) Marginal dose (a) <15 Gy 15 Gy< (b)<20 (c)<20 Gy (P =0.2309) (d) Sex: Male and female (P =0.2704)
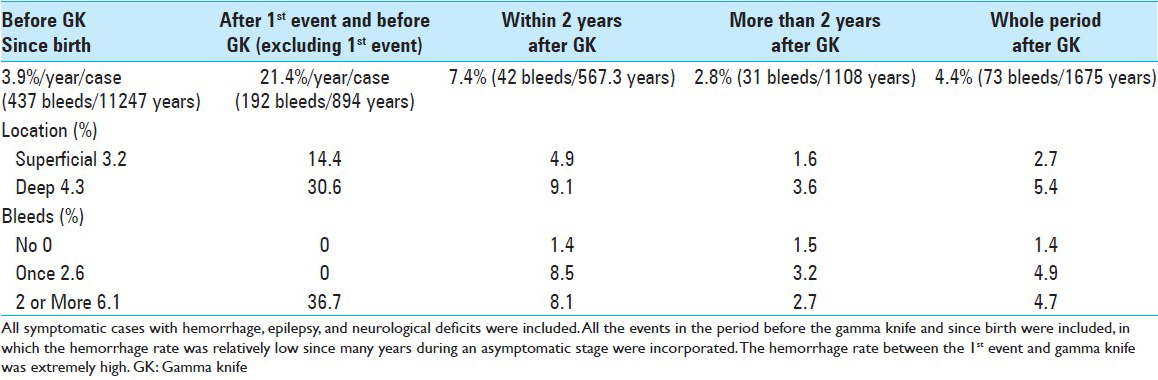
When stratified this by locations and bleeding times, the deeply located lesions and the ones of multiple bleedings demonstrated higher hemorrhage rates before GK treatment. The rates estimated to be 7.4%/year/case within 2 years after radiosurgery and 2.8%/year/case thereafter, resulting in a rate of 4.4% year/case for the entire follow-up period after radiosurgery
When only the 255 cases presenting with hemorrhage as a first episode were analyzed, the hemorrhage rate from the birth (including first episode) was 4.4%/year/case. However, the rate increased to 28.7% during first episode to radiosurgery, in which the first episodes were excluded from the calculation. After radiosurgery, the rate dropped down to 8.4% during the first 2 years, and 3.0% thereafter. Overall hemorrhage rate after radiosurgery was 4.8%/year/case [
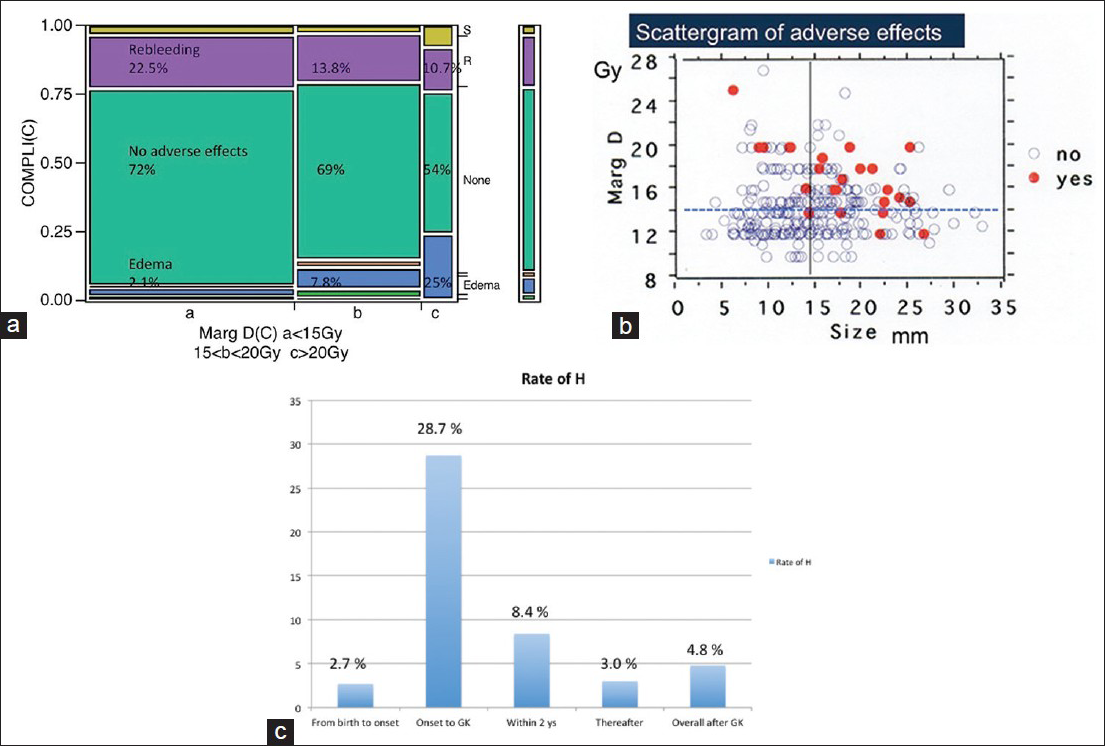
Figure 4
(a)Undesirable events and rebleeding occurring after gamma knife treatment and relation to the marginal dose variations during radiosurgery. (b) Complications occurred more frequently among cases more than 15 mm in diameter and cases treated with more than 15 Gy. (c) Changes of annual hemorrhage rate (AHR). Although AHR since birth to first episode was low, it jumped up to 28.7% during first episode and radiosurgery. The rate gradually dropped down to 8.4% in the first 2 years after radiosurgery and 3.0% thereafter. Overall AHR after radiosurgery was 4.8%/year/case
Seizure control
Seizure outcome data were estimated using Engel's classification. Among 27 cases with sufficient follow-up period of 83 months, 13 of them (48%) were seizure-free (Engel I), but the others remained in class II (26%) or III (26%). Two types of seizure cases were observed: Cases with s-CMs associated with repetitive minor hemorrhages, and cases with s-CMs surrounded by hemosiderin-stained brain tissue without recognizable hemorrhage. Typically, the seizures associated with the former cases were not difficult to control, whereas latter cases were often refractory to treatment. Further treatments, such as surgical resection were thus required in four cases, resulting in excellent seizure control.
Complications
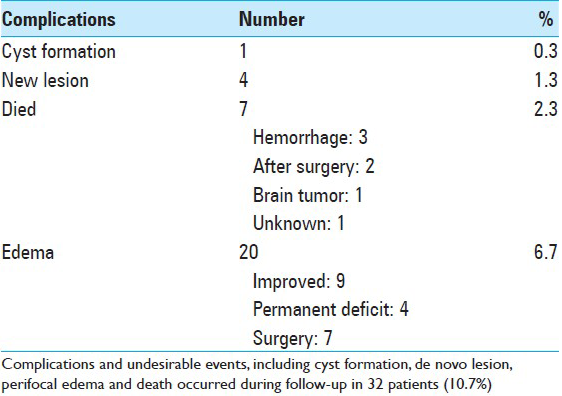
Radiation-induced edema in and around the CM with accompanying neurological signs was the most common complication. In this series, there were 20 cases of symptomatic radiation-induced edema (6.7%) in the surrounding brain tissue. Among them, nine cases were improved and four had permanent deficits. The other seven cases were surgically treated at the time of radiation-induced edema. De novo lesions (1.3%) and/or cyst formation (0.3%) were observed [
Rebleeding
Rebleeding occurred more frequently in the cases treated with the marginal dose less than 15 Gy. Conversely, perifocal edema occurred more frequently in the cases treated with more than 20 Gy [
DISCUSSION
There has been a long-term discussion on how radiosurgery can contribute for the treatment of s-CMs. This study is believed to be the largest series of s-CMs treated with GK and reported in the literature.
Natural history as described in medical literature
Bleedings or seizures caused by intracranial CM seem to be relatively rare, and a majority of such lesions are believed to be asymptomatic over time. In two early reports describing the natural history of CM, Curling et al.[
Natural history of symptomatic cavernous malformations
The natural history of s-CMs is totally different from that of asymptomatic lesions, as frequent hemorrhages or seizures occur after the first event.[
Surgery for s-CMs
Several studies examining surgery for symptomatic lesions associated with hemorrhage or intractable seizure have been reported in the literature.[
Gamma knife treatment for s-CM
With the realization of successful AVM radiosurgery, CMs are now initially treated with GK surgery. However, because of the relatively high complication rate and occasional bleeding even after treatment, such trials have always been controversial and limited.[
Other investigators have described negative results of radiosurgery, [
Although randomized trial for s-CMs is required, it is difficult to accomplish the study because s-CMs are not common. Moreover, it is not adequate to watch the patients suffering from repetitive episode of hemorrhage for long time with conservative treatment.
Surgery and radiosurgery
In order to share light into this controversial dispute, a concurrent retrospective study on the natural history of s-CM, as well as the results of surgery was carried out here. Our data of natural history of pure s-CM as previously mentioned were compared with the results of surgery and radiosurgery. All three were almost comparable in age, sex, and onsets, and carried out with very similar study protocols [
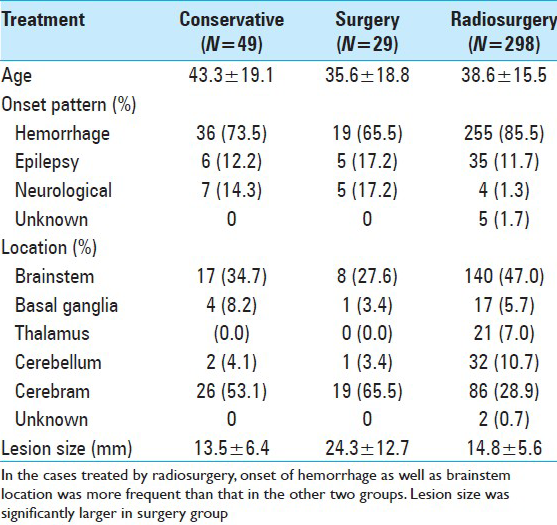
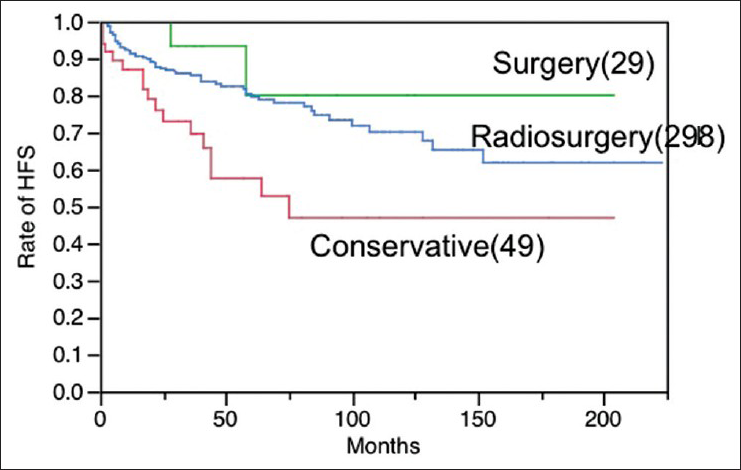
Figure 5
Hemorrhage-free survival after surgery (S) (29 cases), radiosurgery with gamma knife (R) (298 cases) and conservative treatment© (49 cases). The difference of HFS is statistically significant between S and C groups (P=0.0176), as well as R and C groups (P=0.0026), however, not significant between S and R groups (P=0.2489)
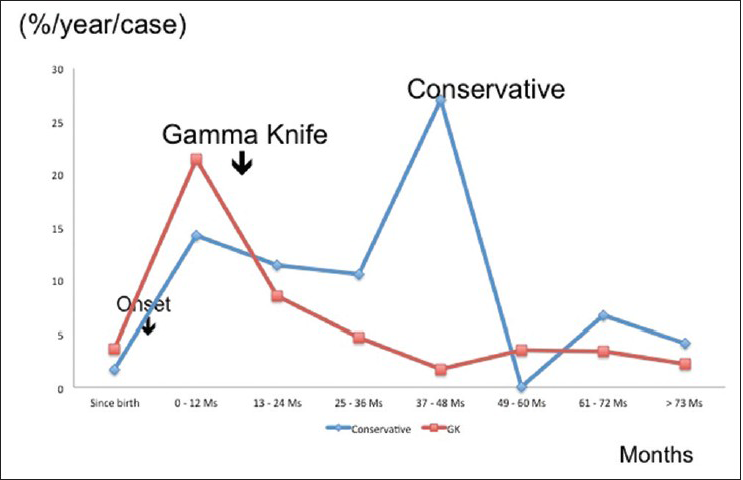
Figure 6
Comparison of annual hemorrhage rate between radiosurgery and conservative groups. Since the mean interval between the onset and radiosurgery was 33 months (mean: 7 months), this time differences were carefully adjusted to zero. The annual hemorrhage rate apparently decreased after radiosurgery when compared with that of conservative treatment for symptomatic cavernous malformations. In the latter (conservative group: 49 cases), hemorrhagic episodes were frequent especially within 5 years after the onset, forming peaks of high hemorrhage rate
Strategy for symptomatic cavernous malformations
Complete surgical resection is ideal for preventing rebleedings. However, the AHR is not superior to that of conservative treatment when only a partial resection is performed. Moreover, serious adverse effects of surgical intervention to the brainstem and basal ganglia may occur. Radiosurgery obviously reduces the hemorrhage rate, and can be used for lesions in the brainstem and deep brain structures. Thus, the treatment strategy for s-CM should not be simple, and a deep understanding of the natural history, neurological status, location as well as the size of the lesion is required. When a small part of CM tissue remains after surgery, radiosurgery seems to be an ideal option in order to prevent further bleedings.
CONCLUSION
Because s-CMs often show aggressive behaviors, adequate treatment is necessary. After radiosurgery, the AHR is significantly lower than that of conservative treatment. GK radiosurgery is an important option, since the adverse effects are less frequent than with surgery, especially for eloquent locations such as the brainstem or basal ganglia. Radiosurgery brings the hemorrhage rate of these lesions at least to that of natural history when safe doses are used. Early intervention with radiosurgery is preferable when a small part of the CM remains after surgery.
Author contributions to the study and manuscript preparation include following. Conception and design: Kida, Hasegawa. Acquisition of data: Kida. Analysis and interpretation of data: Kida, Hasegawa. Critically revising the article: All authors.
ACKNOWLEDGMENTS
Including seven authors, investigators in the 23 GK institutions described below from across Japan that provided the data used are gratefully acknowledged.
Chigasaki Tokusyuukai Hospital, Takai Hospital, Koyou Hospital, Shiroyama Hospital, Mito Gamma House, North Japan Neurosurgical Hospital, Mominoki Hospital, Tominaga Neurosurgical Hospital, Takashima Hospital, Yamagata Kenritu Central Hospital, Akita Cerebrovascular Research Center, Atuzi Neurosurgical Hospital, Shiokawa Hospital, Nagoya Kyoritu Hospital, South Tohoku Medical Clinic, Kotou Memorial Hospital, Saitama Gamma Knife Cente.
References
1. Amin-Hanjani S, Ogilvy CS, Candia GJ, Lyons S, Chapman PH. Stereotactic radiosurgery for cavernous malformations: Kjellberg's experience with proton beam therapy in 98 cases at the Harvard cyclotron. Neurosurgery. 1998. 42: 1229-38
2. Barker FG, Amin-Hanjani S, Butler WE, Lyons S, Ojemann RG, Chapman PH. Temporal clustering of hemorrhages from untreated cavernous malformation of the central nervous system. Neurosurgery. 2001. 49: 15-25
3. Bertalanffy H, Gilsbach JM, Eggert HR, Seeger W. Microsurgery of deep-seated cavernous angiomas: Report of 26 cases. Acta Neurochir (Wien). 1991. 108: 91-9
4. Chang SD, Levy RP, Adler JR, Martin DP, Krakovitz PR, Steinberg GK. Stereotactic radiosurgery of angiographically occult vascular malformations: 14-year experience. Neurosurgery. 1998. 43: 213-21
5. Cohen DS, Zubay GP, Goodman RR. Seizure outcome after lesionectomy for cavernous malformations. J Neurosurg. 1995. 83: 237-42
6. Curling OD, Kelly DL, Elster AD, Craven TE. An analysis of the natural history of cavernous angioma. J Neurosurg. 1991. 75: 702-8
7. Gross BA, Batjer HH, Awad IA, Bendok BR. Brainstem cavernous malformations. Neurosurgery. 2009. 64: E805-18
8. Gross BA, Lin N, Du R, Day AL. The natural history of intracranial cavernous malformations. Neurosurg Focus. 2011. 30: E24-
9. Hauck EF, Barnett SL, White JA, Samson D. Symptomatic braistem cavernomas. Neurosurgery. 2009. 64: 61-70
10. Karlsson B, Kihlstrom L, Lindquist C, Ericson K, Steiner L. Radiosurgery for cavernous malformations. J Neurosurg. 1998. 88: 293-7
11. Kida Y. Radiosurgery for cavernous malformations in basal ganglia, thalamus and brainstem. Prog Neurol Surg. 2009. 22: 31-7
12. Kondziolka D, Lunsford D, Flickinger JC, Kestle JR. Reduction of hemorrhage risk after stereotactic radiosurgery for cavernous malformations. J Neurosurg. 1995. 83: 825-31
13. Kondziolka D, Lunsford LD, Kestle JR. The natural history of cerebral cavernous malformations. J Neurosurg. 1995. 83: 820-4
14. Kupersmith MJ, Kalish H, Epstein F, Berenstein A, Woo H, Jafar J. Natural history of braistem cavernous malformations. Neurosurgery. 2001. 48: 47-53
15. Lee CC, Pan DH, Chung WY, Liu KD, Yang HC, Wu HM. Brainstem cavernous malformations: The role of Gamma Knife surgery. J Neurosurg. 2012. 117: 164-9
16. Liscak R, Vladyka V, Simonova G, Vymazal J, Novotny J. Gamma knife surgery of brain cavernous hemangiomas. J Neurosurg. 2005. 102: 207-13
17. Lunsford LD, Kahn AA, Niranjan A, Kano H, Flickinger JC, Kondziolka D. Stereotactic radiosurgery for symptomatic solotary cerebral cavernous malformations considered high rrisk for resection. J Neurosurg. 2010. 113: 23-9
18. Pollock BE, Garces YI, Stafford SL, Foote RL, Schomberg PJ, Link MJ. Stereotactic radiosurgery for cavernous malformations. J Neurosurg. 2000. 93: 987-91
19. Robinson JR, Awad IA, Little JR. Natural history of the cavernous angioma. J Neurosurg. 1991. 75: 709-14
20. Samii M, Eghbal R, Carvalho GA, Mathies C. Surgical management of braistem cavernomas. J Neurosurg. 2001. 95: 825-32
21. Sindou M, Yada J, Salord F. Functional results after microsurgical resection of brainstem cavernous malformations (retrospective study of a 12 patient series and review of the recent literature). Acta Neurochir (Wien). 2000. 142: 843-52
22. Sola RG, Pulido P, Pastor J, Ochoa M, Castedo J. Surgical treatment of symptomatic cavernous malformations of the brainstem. Acta Neurochir (Wien). 2007. 149: 463-70
23. Steiner L, Karlsson B, Yen CP, Torner JC, Lindquist C, Schlesinger D. Radiosurgery in cavernous malformations: Anatomy of a controversy. J Neurosurg. 2010. 113: 16-22
24. Tarnaris A, Fernandes RP, Kichen ND. Does conservative management for brain stem cavernomas have better long-term outcome?. Br J Neurosurg. 2008. 22: 748-57
25. Wang CW, Liu AL, Zhang J, Sun B, Zhao Y. Surgical management of brainstem cavernous malformations: Report of 137 cases. Surg Neurol. 2003. 59: 444-54
26. Washington CW, McCoy KE, Zipfel GJ. Update on the natural history of cavernous malformations and factors predicting aggressive clinical presentation. Neurosurg Focus. 2010. 29: E7-
27. Weil S, Tew JM, Steiner L. Comparison of radiosurgery and microsurgery for treatment of cavernous malformations of the brain stem. J Neurosurg. 1990. 72: 336A-

