

- Department of Neurological Surgery, Surgical Critical Care, and Emergency Surgery, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania, USA
- Department of Traumatology, Surgical Critical Care, and Emergency Surgery, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania, USA
Correspondence Address:
Neil R. Malhotra
Department of Neurological Surgery, Surgical Critical Care, and Emergency Surgery, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania, USA
DOI:10.4103/2152-7806.196769
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Prateek Agarwal, John F. Burke, Kalil G. Abdullah, Matthew Piazza, Brian P. Smith, Jayesh P. Thawani, Neil R. Malhotra. Stab wound to the intramedullary spinal cord: Presurgical and surgical management options for a retained blade to optimize neurological preservation. 26-Dec-2016;7:
How to cite this URL: Prateek Agarwal, John F. Burke, Kalil G. Abdullah, Matthew Piazza, Brian P. Smith, Jayesh P. Thawani, Neil R. Malhotra. Stab wound to the intramedullary spinal cord: Presurgical and surgical management options for a retained blade to optimize neurological preservation. 26-Dec-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/stab-wound-to-the-intramedullary-spinal-cord-presurgical-and-surgical-management-options-for-a-retained-blade-to-optimize-neurological-preservation/
Date of Submission
29-Jul-2016
Date of Acceptance
19-Sep-2016
Date of Web Publication
26-Dec-2016
Abstract
Background:We present a rare case of an intraparenchymal nonmissile penetrating spinal injury (NMPSI) occurring at the T11 level in a patient presenting without neurological deficit.
Case Description:The patient sustained a knife wound that penetrated the lamina without incurring bony injury and entered the spinal cord at the T11 level. During surgery, the intramedullary penetration of the cord was confirmed, and following surgical removal of the knife, the patient fully recovered without losing any neurological function.
Conclusions:The surgical management of NMPSI in patients who are neurologically intact is controversial. Here, we report surgical excision of a knife that penetrated the spinal cord at the T11 level, without the patient incurring further neurological deterioration.
Keywords: Nonmissile penetrating spinal injury, penetrating spinal trauma, spinal cord injury, stab wounds
INTRODUCTION
Nonmissile penetrating injuries to the spine (NMPSI) are uncommon.[
CASE PRESENTATION
Initial presentation
A 58-year-old male presented to the emergency department neurologically intact, but with a common kitchen knife penetrating the spinal cord at the T11 level. His only complaint was a patchy, vague, and subjective nondermatomal sensory loss in the lower extremities. A computed tomography (CT) image showed that the knife had pierced the right-sided interlaminar space at the T11-T12 level where it fully entered the spinal canal [
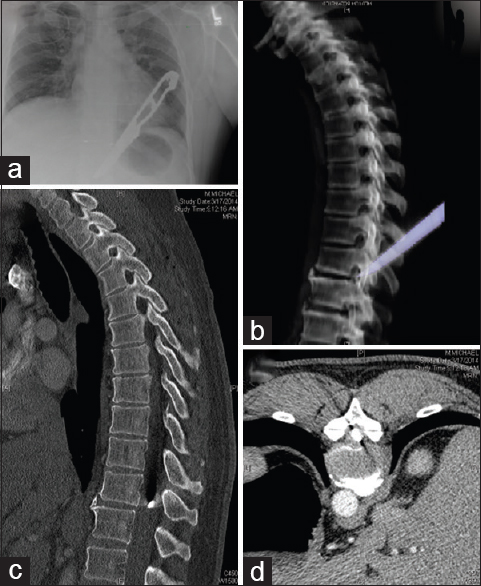
Figure 1
Initial imaging of lesion. (a) Plain films of chest showing knife in the thoracic region. (b) Ghost reconstruction of CT scan showing the knife relative to the vertebral bodies. (c) Sagittal CT of the spine showing the tip of the knife in the intramural space. (d) Axial CT of the spine showing the tip of the knife in the spinal canal
Surgery
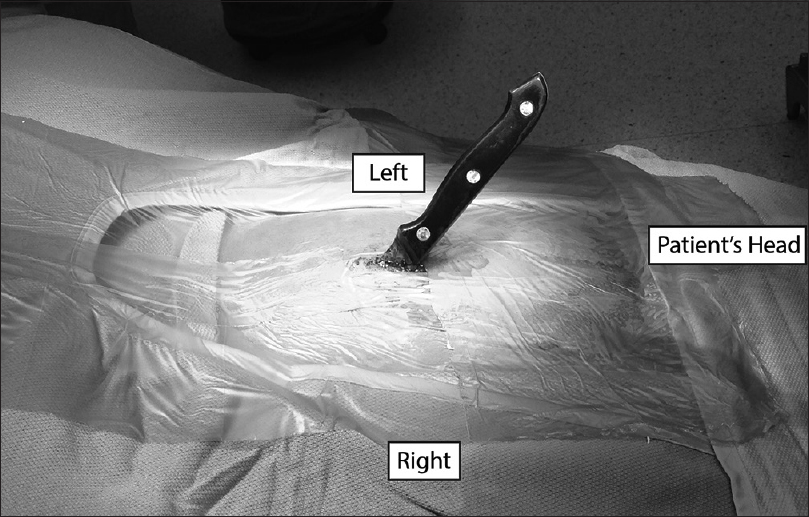
Subsequent to sterile preparation and draping of the patient, the skin was opened perpendicular to the axis of blade, with care being taken to avoid any undue manipulation. In addition, no electrocautery was utilized during dissection and removal of the knife to avoid potential damage to the spinal cord. The serrated knife was firmly embedded in the T11-T12 laminar bone. An ultrasonic bone cutter was used to create a bone island around the knife, allowing the knife and the surrounding T11-T12 laminae to be removed without traumatic rotational force to the spinal cord. Under microscope visualization, the dural laceration from the knife was extended in order to look for intradural compressive hematoma or vascular injury. Although neither was present, there was a clear laceration of the spinal cord itself. Following copious irrigation, watertight dural closure was performed using running 4-0 Nurolon sutures. In order to minimize infection risk given the foreign body penetration, no adjuvant sealant was used, especially because solid dural closure had been achieved. The patient was placed on antibiotics and received a tetanus shot. Postoperatively, the patient's motor status remained normal, whereas his mild diffuse sensory loss was unchanged. Three months later, the patient continued to have residual sensory deficit, but was fully ambulatory and returned to work.
DISCUSSION
Decision making in patients who are neurologically intact but have sustained penetrating spinal trauma is complicated. Evidence for surgical management of penetrating spinal trauma has largely been driven by isolated case reports.[
Without focal neurological findings, it is typically presumed that the spinal cord has not been penetrated, making surgical exploration controversial.[
CONCLUSION
In conclusion, NMPSI with a retained object in a neurologically intact patient does not preclude an intramedullary lesion. Surgical exploration of all such injuries should be performed in order to extract the retained foreign object, utilizing the methods recommended in this case to avoid trauma to the spinal cord.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Enicker B, Gonya S, Hardcastle TC. Spinal stab injury with retained knife blades: 51 Consecutive patients managed at a regional referral unit. Injury. 2015. 46: 1726-33
2. Goyal RS, Goyal NK, Salunke P. Non-missile penetrating spinal injuries. Indian J Neurotrauma. 2009. 6: 81-4
3. Li X, Curry EJ, Blais M, Ma R, Sungarian AS. Intraspinal penetrating stab injury to the middle thoracic spinal cord with no neurologic deficit. Orthopedics. 2012. 35: e770-3
4. Lipschitz R. Associated injuries and complications of stab wounds of the spinal cord. Paraplegia. 1967. 5: 75-82
5. Prasad BC, Vemula RC, Varaprasad G. Nonmissile penetrating spinal injury with an impaled knife: Case report. Indian J Surg. 2013. 75: 237-8
6. Shahlaie K, Chang DJ, Anderson JT. Nonmissile penetrating spinal injury. Case report and review of the literature. J Neurosurg Spine. 2006. 4: 400-8
7. Skadorwa T, Ciszek B. Pediatric arrowshot injury to cervical spinal cord-sagittal cord transection with no neurological deficit and good outcome: Case report and review of literature. Childs Nerv Syst. 2013. 29: 1933-9
8. Thakur RC, Khosla VK, Kak VK. Non-missile penetrating injuries of the spine. Acta Neurochir. 1991. 113: 144-8
9. van den Berg ME, Castellote JM, Mahillo-Fernandez I, de Pedro-Cuesta J. Incidence of spinal cord injury worldwide: A systematic review. Neuroepidemiology. 2010. 34: 184-92
10. Xia X, Zhang F, Lu F, Jiang J, Wang L, Ma X. Stab wound with lodged knife tip causing spinal cord and vertebral artery injuries: Case report and literature review. Spine. 2012. 37: E931-4

