

- Neurosurgery Department, Memfys Hospital for Neurosurgery, Enugu, Nigeria
- Neurosurgery Department, University of Nigeria Teaching Hospital, Enugu, Nigeria
- Enugu State University Teaching Hospital, Enugu, Nigeria
Correspondence Address:
S. Ohaegbulam
Neurosurgery Department, Memfys Hospital for Neurosurgery, Enugu, Nigeria
DOI:10.4103/sni.sni_100_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: S. Ohaegbulam, O. Okwunodulu, C. Ndubuisi, W. Mezue, M. Chikani, S. Nkwerem, M. Ekuma. Vestibular schwannoma appears to be very rare in a region of Sub-Saharan Africa. 01-Aug-2017;8:171
How to cite this URL: S. Ohaegbulam, O. Okwunodulu, C. Ndubuisi, W. Mezue, M. Chikani, S. Nkwerem, M. Ekuma. Vestibular schwannoma appears to be very rare in a region of Sub-Saharan Africa. 01-Aug-2017;8:171. Available from: http://surgicalneurologyint.com/surgicalint-articles/vestibular-schwannoma-appears-to-be-very-rare-in-a-region-of-sub%e2%80%91saharan-africa/
Date of Submission
09-Mar-2017
Date of Acceptance
12-Apr-2017
Date of Web Publication
01-Aug-2017
Abstract
Background:Vestibular schwannoma (VS) is a significant neurosurgical problem hence it enjoys a special attention at conferences and workshops. It accounts for about 8–10% of all intracranial tumors with an annual incidence of about 11–14 per million per year. Most VS are sporadic with 5–10% attributed to neurofibromatosis type 2 (NF2). However, VS is alleged to be rare in Africans and uncommon in African Americans, connoting a racial bias. To our knowledge, no study from sub-Saharan Africa has addressed this subject. The aim of this study is to determine the frequency of VS in a tertiary neurosurgical hospital in sub-Saharan Africa.
Methods:This is a retrospective study of all intracranial neoplasms and VS managed in a major tertiary hospital in sub-Saharan Africa from January 2003 to December 2015. Patients’ records and neuroimaging studies were reviewed retrospectively. Additionally, database of all cranial computed tomography (CT) and magnetic resonance imaging (MRI) done for various indications within the same period was searched retrospectively for “incidental” VS cases.
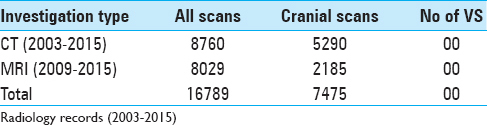
Results:Over the study period of 13 years, out of 612 cases of intracranial neoplasms, only three (0.49%) were VSs (two sporadic, one bilateral VS in NF2). A search for “incidental” cases of VS from a pool of 7475 cranial scans (CT: 5290; MRI: 2185), yielded none.
Conclusions:The findings strongly suggest that VS is very rare in the study population. It is hoped that other centers in Africa and beyond would perform similar studies.
Keywords: Intracranial tumors, geographical neurosurgery, neurofibromatosis, vestibular schwannoma
INTRODUCTION
Vestibular schwannoma (VS), commonly termed acoustic neuroma, arises on the eighth cranial nerve and accounts for about 8–10% of all intracranial tumors, with an annual incidence of about 11.8–14 per million per year.[
Hearing loss is the most common presenting symptom due to compression of adjacent cochlear nerve. Most VS are sporadic, but 5-13% are associated with NF2, which is an autosomal dominant disorder characterized by bilateral VS, other CNS tumors, and characteristic growth rate of VS.[
The incidence rates of VS vary worldwide from 1 to 20 cases per million inhabitants per year, and is reported to be on the increase globally.[
The aim of this study is to determine the frequency of VS in a major neurosurgical hospital in south east Nigeria.
MATERIALS AND METHODS
This is a retrospective study of all cases of VS diagnosed at the study tertiary hospital over a 13-year period (1 January 2003 to 31 December 2015). The medical records, CT, MRI, and histopathology records were used. Additionally, database of all cranial CT and MRI done for various indications within the same period was searched for “incidental” cases of VS. The hospital is the main referral neurosurgical hospital serving the city (population 722,664) as well as all the neighboring cities and states with a catchment population of over 20 million. The hospital also offers CT, MRI, neurology, and neurosurgery services.
RESULTS
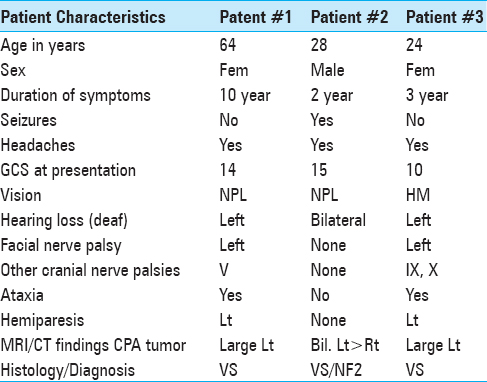
During the study period, 612 patients with intracranial tumors were diagnosed out of which there were two cases of sporadic VS and a case of bilateral VS or NF2 [
Search for “incidental” VS
This was accomplished through the search of the database of all cranial CTs and MRIs performed at the hospital between 2003 and 2015. From the 7475 cranial scans (CT: 5290; MRI: 2185), no “incidental” cases of VS were found [
DISCUSSION
Spanning over a period of 13 years, out of 612 cases of intracranial neoplasms, only three (0.49%) were VS. This was undoubtedly a rather small proportion of all intracranial neoplasms managed at the institution during the study period. The patient population consisted of black Africans of predominantly single ethnicity, suggesting that VS is rare in this part of Africa and may have a racial bias. An earlier study of intracranial tumors from the same area also reported no cases of VS.[
Schwannomas actually represent 8–10% of all intracranial neoplasms, but this frequency appears to have a racial bias.[
In a review of the clinical characteristics of 4886 adult patients who underwent acoustic neuroma excision in the USA, it was reported that 85.4% were Caucasians while only 3.7% were African Americans.[
It is possible that asymptomatic lesions may account for the relative rarity of VS in this study and amongst black people in general. However, the zero “incidental” VS in this study despite the relatively large sample size suggests the rarity of VS in this study black population. This is in sharp contrast to the findings in the retrospective analysis of MRI scans by Lin et al.[
The question then arises as to why VS should be rare in this study population when the incidence is rising in other parts of the world. In the search for an answer, it is appropriate to examine some of the etiological factors that have been incriminated in the pathogenesis of VS which include loud noise and use of mobile phones.[
A large nationwide cohort study in Denmark revealed that high level of education and high disposable income were associated with the occurrence of VS in both sexes.[
VS causes impaired hearing and one would expect that anybody who experiences progressive deafness would seek medical help at the earliest opportunity. Educated people are more likely to recognize early deafness because of increased communication needs. Paradoxically, it is known that tumor size is not always directly proportional to the degree of hearing impairment since large VS may cause mild hearing loss while small tumors may cause marked deafness.
Late presentation is a common phenomenon in Africa hence intracranial tumors reach giant size before diagnosis. In a recent analysis of pituitary tumors, about 30% of the patients were already giant tumors by the time of presentation.[
Are there genetic factors to be considered as possible reasons for the rarity of VS in the study population? It is known that VS is due to loss of tumor suppressor gene on the long arm of chromosome 22. This is a somatic mutation in sporadic cases of VS, but in NF2 this is an inherited abnormality or a new mutation that is transmitted to the offspring.
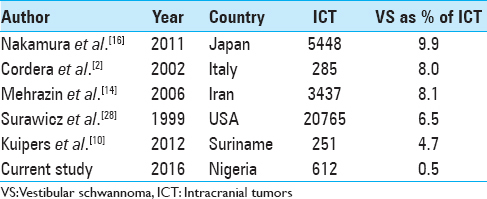
Given the increase in the availability of neuroimaging and neurosurgical services in our locality as in other parts of Africa, the prevalence of VS has not displayed rising trends. A study of the global frequency of VS in intracranial tumor series demonstrates this difference [
CONCLUSION
Vestibular schwannoma seems to be rare in the study population. This finding strengthens the belief that VS exhibits racial bias with relative rarity in blacks. If this is confirmed from other researchers, the quest for the factors that protect some people from VS should be intensified as this could ultimately lead to prevention and even cure.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors gratefully acknowledge the contributions of the radiology department, the pathologists for reporting on the excised tumors and the ethics committee of the hospital.
References
1. Abaza MM, Makariou E, Armstrong M, Lalwani AK. Growth rate characteristics of acoustic neuromas associated with Neurofibromatosis type 2. Laryngoscope. 1996. 106: 674-9
2. Cordera S, Bottachi E, D’Alessandro G, Machado D, Gonda F, Corso G. Epidemiology of primary intracranial tumours in NW Italy, a population based study: Stable incidence in the last two decades. J Neurol. 2002. 249: 281-4
3. Curry WT, Barker FG. Racial, ethnic and socioeconomic disparities in the treatment of brain tumours. J Neurooncol. 2009. 93: 25-39
4. Edwards CG, Schwartzbaum JA, Lönn S, Ahlbom A, Feychting M. Exposure to loud noise and risk of acoustic neuroma. Am J Epidemiol. 2006. 163: 327-33
5. Edwards CG, Schwartzbaum JA, Nise G, Forssén UM, Ahlbom A, Lönn S. Occupational noise exposure and risk of vestibular schwannoma. Am J Epidemiol. 2007. 166: 1252-8
6. Evans DG, Moran A, King A, Saeed S, Gurusinghe N, Ramsden R. Incidence of vestibular schwannoma and Neurofibromatosis 2 in the North West of England over a 10-year period; higher incidence than previously thought. Otol Neurotol. 2005. 26: 93-7
7. Hoffman S, Propp JM, McCarthy BJ. Temporal trends in incidence of primary brain tumours in the United States, 1985–1999. Neurooncol. 2006. 8: 27-37
8. Howitz MF, Johansen C, Tos M, Charabi S, Olsen JH. Incidence of vestibular schwannoma in Denmark, 1977-1995. Am J Otol. 2000. 21: 690-4
9. Jeyakuma A, Seith R, Brickman TM, Dutcher P. The prevalence and clinical course of patients with ‘incidental’ acoustic neuromas. Acta Otolaryngol. 2007. 127: 1051-7
10. Kuipers SE, Kafiluddin E, Joe RT, Peerdeman S. Incidence and treatment of Central Nervous System Tumours in Suriname. World Neurosurg. 2013. 80: e79-83
11. Lanser MJ, Sussman SA, Frazer K. Epidemiology, pathogenesis, and genetics of acoustic tumours. Otolaryngol Clin North Am. 1992. 25: 499-520
12. Lin D, Hegarty JL, Fischbein NJ, Jackler RK. The prevalence of ‘Incidental’ Acoustic Neuroma. Arch Otolaryngol Head Neck Surg. 2005. 131: 241-4
13. McClelland S, Guo H, Okuyemi KS. Morbidity and mortality following acoustic neuroma excision in the United States: Analysis of racial disparities during a decade in the radiosurgery era. Neurooncol. 2011. 13: 1252-9
14. Mehrazin M, Rahmat H, Pavari P. Epidemiology of primary intracranial tumours in Iran, 1978-2003. Asian Pac J Cancer Prev. 2006. 7: 284-8
15. Mezue WC, Ohaegbulam SC, Chikani MC, Achebe DN. Management of Giant Pituitary Tumours Affecting Vision in Nigeria. World Neurosurg. 2012. 77: 606-9
16. Nakamura H, Makino K, Yano S, Kuratsu J. Epidemiological study of primary intracranial tumours: A regional survey in Kumamoto Prefecture in southern Japan-20-year study. Int J Clin Oncol. 2011. 16: 314-21
17. Ohaegbulam SC, Saddeq N, Ikerionwu S. Intracranial Tumours in Enugu, Nigeria. Cancer. 1980. 46: 2322-4
18. Olayinka OS. Effective noise control measures and sustainable development in Nigeria. World J Environmental Engineering. 2013. 1: 5-15
19. Preston-Martin S, Thomas DC, Wright WE, Henderson BE. Noise trauma in the aetiology of vestibular schwannomas in men in Los Angeles County, 1978–1985. Br J Cancer. 1989. 59: 783-6
20. Propp JM, McCarthy BJ, Preston-Martin S. Descriptive epidemiology of vestibular schwannomas. Neuro Oncol. 2006. 8: 1-11
21. Saadu AA, Onyeonwu RO, Ayorinde EO, Ogisi FO. Road traffic noise survey and analysis in some major Urban centres in Nigeria. Noise Control Eng J. 1998. 46: 146-58
22. Sarma S, Sekhar LN, Schessel DA. Nonvestibular schwannomas of the brain, a 7-year experience. Neurosurgery. 2002. 50: 437-49
23. Schoemaker MJ, Swerdlow AJ, Auvinen A, Christensen HC, Feychting M, Johansen C. Medical history, cigarette smoking and risk of vestibular schwannoma: An international case–control study. Int J Cancer. 2007. 120: 103-10
24. Schüz J, Jacobsen R, Olsen JH, Boice JD, McLaughlin JK, Johansen C. Cellular telephone use and cancer risk: Update of a nationwide Danish cohort. J Natl Cancer Inst. 2006. 98: 1707-13
25. Schüz J, Marianne S, Søren H, Sven-Eric S, Per CT, Christoffer J. Sociodemographic factors and vestibular schwannoma: A Danish nationwide cohort study. Neuro Oncol. 2010. 12: 1291-9
26. Seedat RY, Claassen AJ, Mol DA. Incidence and management of acoustic neuromas in South Africa. Otol Neurotol. 2002. 23: 996-8
27. Simpson RH, Sparrow OC, Duffield MS. Cerebellopontine angle tumours in black South Africans-how rare are acoustic schwannomas?. S Afr Med J. 1990. 78: 11-4
28. Surawicz TS, McCarthy BJ, Kupelian V, Jukich PJ, Bruner JM, Davis FG. Descriptive epidemiology of primary brain and CNS tumours: Results from the Central Brain Tumour Registry of the United States, 1990-1994. Neuro Oncol. 1999. 1: 14-25
29. Tos M, Stangerup SE, Cayé-Thomasen P, Tos T, Thomsen J. What is the real incidence of vestibular schwannoma?. Arch Otolaryngol Head Neck Surg. 2004. 130: 216-20
30. Weller RO, Cervos-Navarro J, Gowing NFC.editors. Pathology of peripheral nerves. Tumour Histopathology. London: Butterworths; 1977. p.

