

- Department of Neurosurgery, Saiseikai Shiga Hospital, Ritto, Shiga, Japan.
Correspondence Address:
Takuma Aoki, Department of Neurosurgery, Saiseikai Shiga Hospital, Ritto, Shiga, Japan.
DOI:10.25259/SNI_479_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Takuma Aoki, Yukihiro Goto, Yujiro Komaru, Shigeomi Yokoya, Hideki Oka. Massive intracerebral hemorrhages due to peripheral middle cerebral artery aneurysm rupture: A case report with a surgical video. 16-Aug-2021;12:412
How to cite this URL: Takuma Aoki, Yukihiro Goto, Yujiro Komaru, Shigeomi Yokoya, Hideki Oka. Massive intracerebral hemorrhages due to peripheral middle cerebral artery aneurysm rupture: A case report with a surgical video. 16-Aug-2021;12:412. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11044
Date of Submission
14-May-2021
Date of Acceptance
24-Jul-2021
Date of Web Publication
16-Aug-2021
Abstract
Background: Saccular aneurysm in the distal segment of the middle cerebral artery (DMCA) occurs very rarely and often represents with a rupture. We report a successful surgical case of a DMCA aneurysm rupture with large cerebral and subarachnoid hemorrhage.
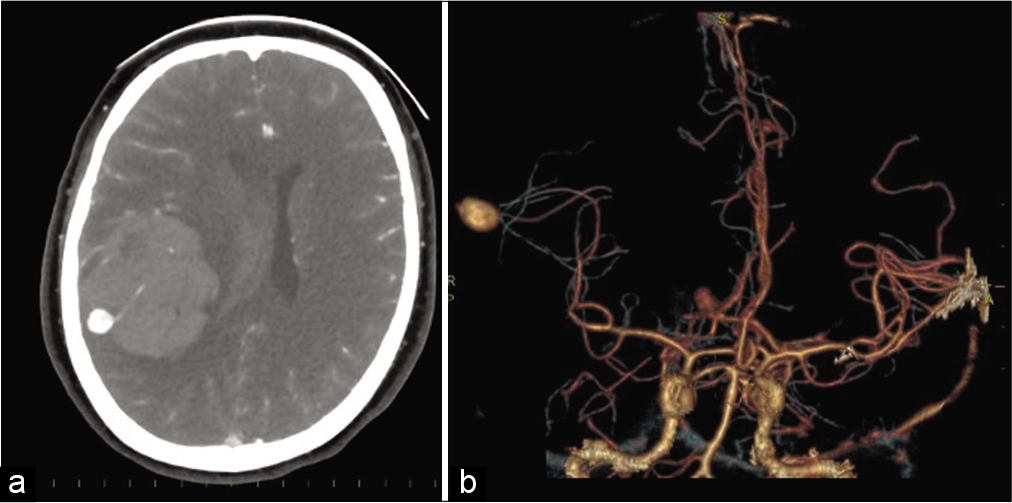
Case Description: A 44-year-old female presented a sudden onset headache and coma (the Glasgow Coma Scale was 3). Head computed tomography (CT) revealed a subarachnoid hemorrhage around the right Sylvian fissure and large intracranial hematoma in the right parietal lobe. The CT angiography showed a saccular aneurysm in the peripheral cortical segment of the right angular branch of the right DMCA. We decided to perform a right craniotomy to evacuate hematoma and interrupt the aneurysm. Just after the dural incision, the aneurysm ruptured again. We applied a temporary clip on the artery proximal to the aneurysm before excising it.
Conclusion: Aneurysm in DMCA can be treated safely with surgical excision and risk of sudden recurrent hemorrhage needs to be anticipated.
Keywords: Distal middle cerebral artery aneurysm, Intracerebral hemorrhage, Surgery video
INTRODUCTION
Saccular aneurysm in the distal segment of the middle cerebral artery (DMCA) without a bacterial origin is a very rare occasion, consisting 1.1–7% of all middle cerebral artery (MCA) aneurysms. Little is known regarding its natural history or its management. Herein, we report a case of DMCA rupture without a bacterial origin accompanied by a large intracerebral hemorrhage and needed microsurgical excision of the aneurysm and evacuation of hematoma.
CASE PRESENTATION
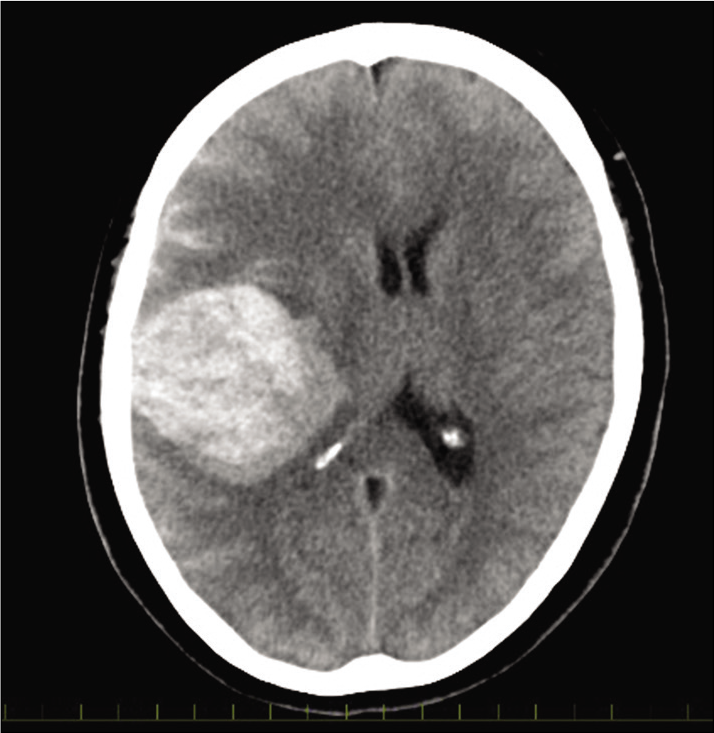
A 44-year-old female presented with a severe, sudden onset headache accompanied by vomiting. She had no history of head trauma, infectious disease, and hypertension. Upon admission, the patient’s Glasgow Coma Scale (GCS) score was 3. Routine blood analysis performed immediately upon admission was normal. Cardiac ultrasound examination revealed no valvular disease or any other abnormal findings. Neurological examination revealed left hemiplegia and right pupil dilation. Head computed tomography (CT) revealed a subarachnoid hemorrhage around the right Sylvian fissure and large intracranial hematoma (ICH) in the right parietal lobe [
A right craniotomy was done immediately to evacuate the ICH and excise the aneurysm. Following dural incision, a massive arterial hemorrhage occurred due to re-ruptured of the aneurysm. We applied a temporary clip proximal to the aneurysm to stop the bleeding. We checked both proximal and distal arterial courses of the aneurysm, confirmed a limited blood supply within the cerebral cortex with ICH, and removed the aneurysm from the angular artery [ Video 1 ].
Video 1
Therapeutic approaches for cerebral vasospasm following SAH post-surgery included ventricular drainage, induced hypertension and blood volume expansion, and antiplatelet therapy. Post-operatively, left hemiplegia recovered gradually with physical rehabilitation. The patient was discharged from the hospital 8 weeks after admission with GCS of 15 and classified as grade 3 on the modified Rankin scale.
DISCUSSION
PMCA without a bacterial origin is very rare condition, consisting 1.1–7% of all MCA aneurysms.[
Concerning its high rebleeding rate, some reports referred an association between rebleeding and the external ventricular drainage, which is an effective treatment to immediately decrease intracranial pressure (ICP). A sudden ICP decrease may be related to rebleeding. This fit to our case, in which rebleeding was seen following craniotomy.
Progression in the field of endovascular treatment (EVT) enables surgeons to treat PMCA rupture.[
CONCLUSION
Here, we report a successful treatment of a PMCA rupture with a large ICH. We have to be ready to perform microsurgery promptly in the case of rebleeding.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video available on:
www.surgicalneurologyint.com
References
1. Ahn JY, Han IB, Joo JY. Aneurysm in the penetrating artery of the distal middle cerebral artery presenting as intracerebral haemorrhage. Acta Neurochir (Wien). 2005. 147: 1287-90
2. Calvacante T, Derrey S, Curey S, Langlois O, Fréger P, Gérardin E. Distal middle cerebral artery aneurysm: A proposition of microsurgical management. Neurochirurgie. 2013. 59: 121-7
3. Dashti R, Hernesniemi J, Niemelä M, Rinne J, Lehecka M, Shen H. Microneurosurgical management of distal middle cerebral artery aneurysms. Surg Neurol. 2007. 67: 553-63
4. Elsharkawy A, Lehečka M, Niemelä M, Billon-Grand R, Lehto H, Kivisaari R. A new, more accurate classification of middle cerebral artery aneurysms: Computed tomography angiographic study of 1, 009 consecutive cases with 1, 309 middle cerebral artery aneurysms. Neurosurgery. 2013. 73: 94-102
5. Lv N, Zhou Y, Yang P, Li Q, Zhao R, Fang Y. Endovascular treatment of distal middle cerebral artery aneurysms: Report of eight cases and literature review. Interv Neuroradiol. 2016. 22: 12-7

