

- Spinal Disorders Center, Fujieda Heisei Memorial Hospital, Fujieda, Shizuoka, Kanagawa, Japan.
- Department of Neurosurgery, Kitasato University School of Medicine, Sagamihara, Kanagawa, Japan.
Correspondence Address:
Wakiko Saruta, Spinal Disorders Center, Fujieda Heisei Memorial Hospital, Fujieda, Shizuoka, Japan.
DOI:10.25259/SNI_611_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Wakiko Saruta1, Toshiyuki Takahashi1, Toshihiro Kumabe2, Manabu Minami1, Ryo Kanematsu1, Hiroya Shimauchi Ohtaki1, Ryotaro Otsuka1, Junya Hanakita1. Transdural reduction of a bone fragment protruding into the spinal canal during surgical treatment of lumbar burst fracture: A case report. 16-Aug-2021;12:406
How to cite this URL: Wakiko Saruta1, Toshiyuki Takahashi1, Toshihiro Kumabe2, Manabu Minami1, Ryo Kanematsu1, Hiroya Shimauchi Ohtaki1, Ryotaro Otsuka1, Junya Hanakita1. Transdural reduction of a bone fragment protruding into the spinal canal during surgical treatment of lumbar burst fracture: A case report. 16-Aug-2021;12:406. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11050
Date of Submission
19-Jun-2021
Date of Acceptance
18-Jul-2021
Date of Web Publication
16-Aug-2021
Abstract
Background: There have been many reports on the clinical, radiographic, and surgical management of thoracolumbar burst fractures attributed to high-energy trauma. Interestingly, few reports have described how to extract bone fragments associated with these injuries protruding into the spinal canal contributing to significant neurological deficits.
Methods: An 18-year-old male presented with a severe L3-level paraparesis (i.e., loss of motor/sensory function below L3 lower extremity hyporeflexia, and sphincter dysfunction: American Spinal Injury Association [ASIA] Impairment Scale B) following a high-speed crash. The computed tomography and magnetic resonance studies revealed a L3 burst fracture with bone fragments protruding into the spinal canal causing marked cauda equina compression. Following a L3-L4 laminectomy, and opening of the dorsal dura, the bone fragments were ventrally impacted into the fractured L3 vertebral body a pedicle/screw L1-L5 fusion was then completed.
Results: One month later, the patient recovered to an ASIA Scale of C, (i.e., residual proximal 3/5 and distal 2/5 motor deficits, with partial sensory sparing).
Conclusion: Transdural ventral impaction of protruded bone fragments attributed to high speed lumbar burst fractures contributing to significant cauda equina compression can be safely/effectively accomplished.
Keywords: Cauda equina injury, Lumbar burst fracture, Spinal fixation, Transdural decompression
INTRODUCTION
Lumbar burst fractures caused by high-energy trauma, can result in vertebral body bone fragments protruding into the spinal canal, resulting in significant cauda equina/root injuries.[
MATERIALS AND METHODS
History and examination
An 18-year-old male fell from a height of 10 m resulting in an L3-level paraparesis (i.e., complete motor loss, partial sensory loss, and sphincter dysfunction: American Spinal Injury Association Impairment Scale B) [
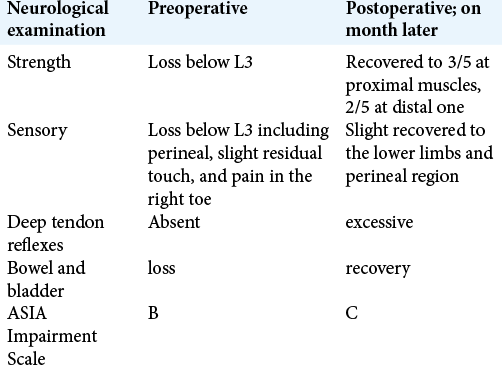
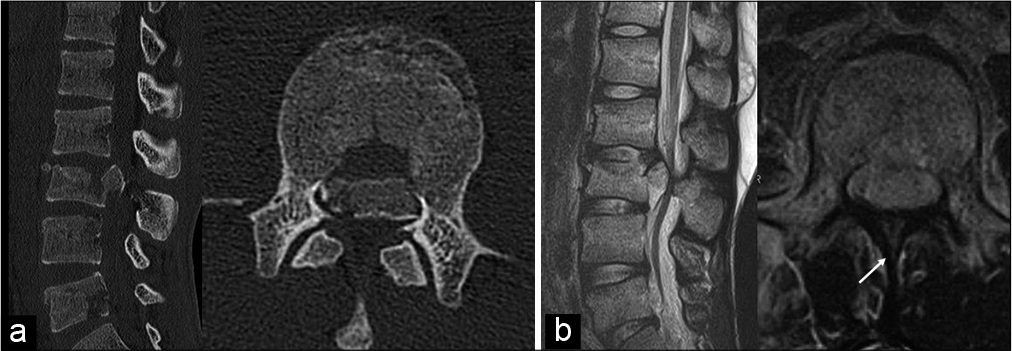
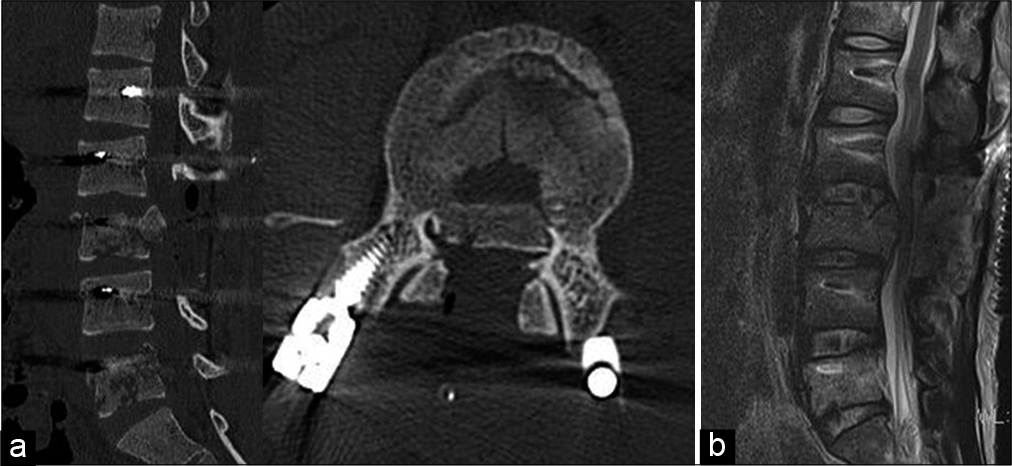
Figure 1:
Preoperative computed tomography (CT) and magnetic resonance imaging (MRI). (a) CT revealed a fracture of the L3 vertebra. (b) Sagittal and axial T2-weighted image demonstrated severe dural sac impingement between a protruded bone fragment of the vertebral body and a fractured spinous process, with remarkable compression of cauda equina. The spinous process was fractured and the rootlets were deviated (white arrow).
Operative procedure
Performing a L3-L4 laminectomy, revealed his dorsal dura was lacerated, with several damaged nerve rootlets herniating through the traumatic durotomy [
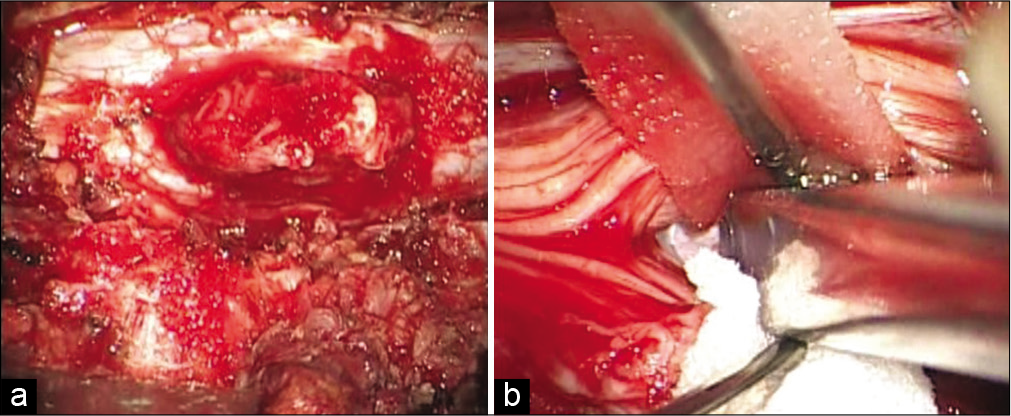
Figure 2:
Intraoperative photographs. (a) The dorsal dura mater was found to be lacerated and several damaged rootlets herniated from the point of the ruptured dura mater. (b) The protruded bone fragment was pushed back into the ventral side by transdural tapping using an impactor, while protecting the cauda equina.
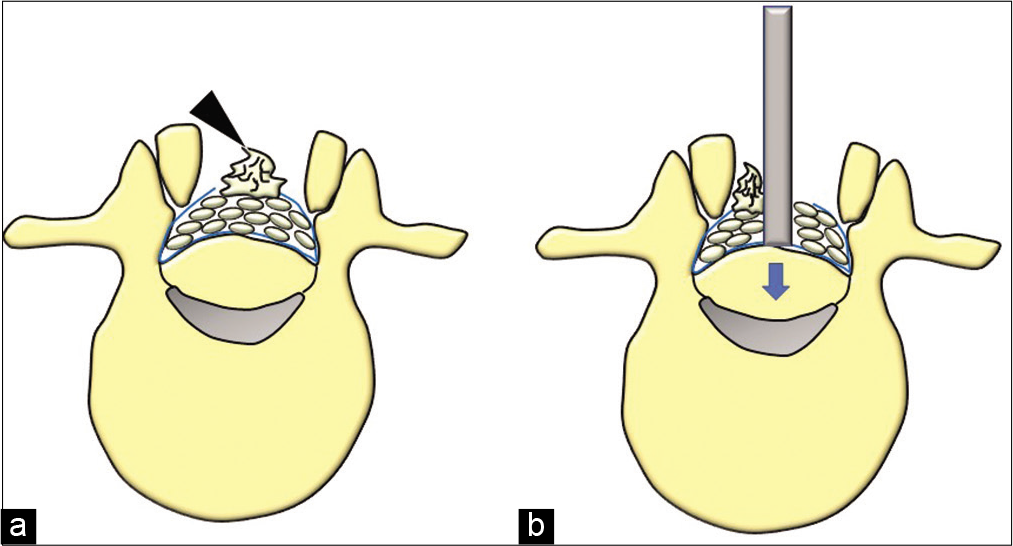
Figure 3:
Illustrations demonstrating the transdural tapping approach. (a) The dural sac was elevated due to the bone fragment from the ventral side. The dorsal dural sac was injured and the rootlets was deviated (arrow head). (b) Transdural tapping, which involves pushing the bone fragment back into the vertebral body.
RESULTS
One month postoperatively, the patient’s proximal (3/5) and distal (2/5) motor strength improved along with bladder and bowel dysfunction completely. Further, the postoperative CT and MRI studies confirmed adequate canal decompression with just a slight residual ventral shift in the protruded bone fragments [
DISCUSSION
Several studies have reported the removal of bone fragments protruding into the spinal canal in patients who have sustained lumbar burst fractures with resultant cauda equina syndromes.[
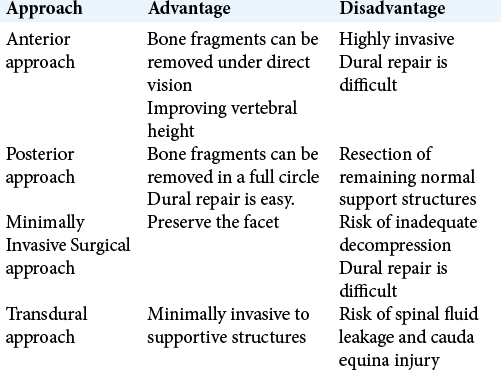
Advantages of posterior versus anterior approach
There are pros and cons for posterior versus anterior approaches to lumbar burst fractures with ventrally extruded/fractured bone fragments contributing to cauda equina syndrome. The posterior approach allows for ventral fragment removal (i.e., tamping down into the fractured vertebral body) while also facilitating direct dorsal dural repair.[
Dural injury due to lumbar vertebral burst fractures
Yoshiiwa et al. found that the cauda equina notch sign was a predictable MR finding of cauda equina entrapment (i.e., due to greenstick lamina fractures), but in many cases this is just found intraoperatively.[
Surgery
Minimally Invasive Surgical (MIS) Approaches: MIS surgical approaches are ineffective when dealing with dorsal dural injuries attributed to lumbar burst fractures. Chen et al. reported ventral packing of fractured fragments under endoscopy with vertebroplasty.[
Transdural Approach to Impaction Vertebral Body Burst Fracture Fragments Contributing to Cauda Equina Compression.
One study discussed impaction of ventral vertebral body bone fragments utilizing a transdural approach in a case in which there was a traumatic dorsal durotomy.[
CONCLUSION
Transdural reduction of protruded lumbar bone fragments through a posterior traumatic durotomy following a L3 burst fracture was safely/effectively accomplished.
Ethical approval
This study was approved by the Medical Ethnic Board of Fujieda Heisei Memorial Hospital (approved number FHR2020-6).
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study
Financial support and sponsorship
Nil
Conflict of Interest
The authors declare that they have no conflict of interest.
References
1. Chen L, Liu H, Hong Y, Yang Y, Hu L. Minimally invasive decompression and intracorporeal bone grafting combined with temporary percutaneous short-segment pedicle screw fixation for treatment of thoracolumbar burst gracture with neurological deficits. World Neurosurg. 2020. 135: e209-20
2. Daisuke I. Bone fragment removal by posterior approach for delayed paralysis due to vertebral body rupture fracture. Orthop Traumatol. 2019. 68: 601-5
3. Deqing L, Kejian L, Teng L, Weitao Z, Dasheng L. Does the fracture fragment at the anterior column in thoracolumbar burst fractures get enough attention?. Medicine (Baltimore). 2017. 96: e5936
4. Haiyun Y, Rui G, Shucai D, Zhanhua J, Xiaolin Z, Xin L. Three-column reconstruction through single posterior approach for the treatment of unstable thoracolumbar fracture. Spine (Phila Pa 1976). 2010. 35: 295-302
5. Lenehan B, Street J, Kwon BK, Noonan V, Zhang H, Fisher CG. The epidemiology of traumatic spinal cord injury in British Columbia, Canada. Spine (Phila Pa 1976). 2012. 37: 321-9
6. Qian Y, Jin C, He L, Zhu GQ, Xu GJ. Anterior reconstruction via a relatively noninvasive retroperitoneal approach for lumbar burst fracture. Orthop Surg. 2015. 7: 185-6
7. Ushiku C, Suda K, Matsumoto S, Komatsu M, Takahata M, Iwasaki N. Dural penetration caused by a vertebral bone fragment in a lumbar burst fracture: A case report. Spinal Cord Ser Cases. 2017. 3: 2016-8
8. Wang Y, Ning C, Yao L, Huang X, Zhao C, Chen B. Transforaminal endoscopy in lumbar burst fracture: A case report. Medicine (Baltimore). 2017. 96: e8640
9. Xu JG, Zeng BF, Zhou W, Kong WQ, Fu YS, Zhao BZ. Anterior Z-plate and titanic mesh fixation for acute burst thoracolumbar fracture. Spine (Phila Pa 1976). 2011. 36: e498-504
10. Yoshiiwa T, Miyazaki M, Kodera R, Kawano M, Tsumura H. Predictable imaging signs of cauda equina entrapment in thoracolumbar and lumbar burst fractures with greenstick lamina fractures. Asian Spine J. 2014. 8: 339-45

