

- Department of Neurosurgery, Emory University, Atlanta, Georgia, United States,
- Department of Otolaryngology, Emory University, Atlanta, Georgia, United States.
Correspondence Address:
J. Manuel Revuelta Barbero, Department of Neurosurgery, Emory University, Atlanta, Georgia, United States.
DOI:10.25259/SNI_1173_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: J. Manuel Revuelta Barbero1, Rima S. Rindler1, Clara Martin1, Marcelo Orellana1, Edoardo Porto1, C. Arturo Solares2, Gustavo Pradilla1. Keyhole supraorbital eyebrow approach for the resection of a tuberculum sellae meningioma with intraoperative endoscopic assistance. 18-Mar-2022;13:93
How to cite this URL: J. Manuel Revuelta Barbero1, Rima S. Rindler1, Clara Martin1, Marcelo Orellana1, Edoardo Porto1, C. Arturo Solares2, Gustavo Pradilla1. Keyhole supraorbital eyebrow approach for the resection of a tuberculum sellae meningioma with intraoperative endoscopic assistance. 18-Mar-2022;13:93. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11455
Date of Submission
25-Nov-2021
Date of Acceptance
15-Feb-2022
Date of Web Publication
18-Mar-2022
Abstract
Background: Tuberculum sellae meningiomas represent approximately 5–10% of intracranial meningiomas.[
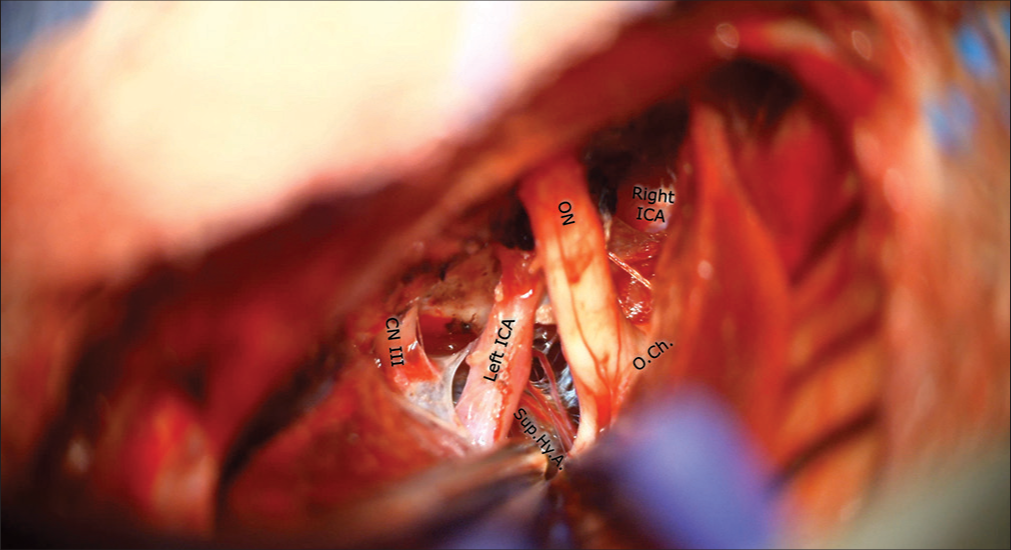
Case Description: The authors report the case of a 42-year-old female who presented with acute-onset vision loss and only finger counting in her left eye associated with headache. Magnetic resonance imaging (MRI) showed a suprasellar extra-axial T1 enhancing mass with encasement of the left optic nerve and paraclinoid internal carotid artery and mass effect on the optic chiasm. A keyhole supraorbital eyebrow approach assisted with a microinspection tool was performed for tumor resection and optic nerve decompression. A Simpson Grade 2 tumor resection was achieved, and histopathology revealed a WHO Grade-I tuberculum sellae meningioma. The patient’s presentation, rationale, key surgical steps, and outcome are discussed, and informed consent for surgery and video recording was obtained.
Conclusion: This surgical video illustrates the use of a keyhole supraorbital eyebrow approach assisted with a microinspection endoscopic tool for the resection of a tuberculum sellae meningioma. The tumor size, extension, and preoperative clinical status determine the optimal surgical corridor in tuberculum sellae meningioma. The keyhole supraorbital eyebrow approach allows safe and direct access to anterior cranial fossa lesions.
Keywords: Keyhole approach, Minimal invasive approach, Supraorbital craniotomy, Tuberculum sellae meningioma
Video 1
Annotations[1-3]
0:00 – Introduction 0:12 – Clinical presentation 0:27 – Neurological examination 0:44 – Neuroimaging findings 1:01 – Rationale for the procedure 1:26 – Risks of the procedure and its potential benefits 1:43 – Alternatives/Why they were not chosen 1:59 – Description of the setup 2:28 – Key surgical steps 2:52 – Operative video 4:50 – 6:11 – Review of clinical and imaging outcome.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
C. Arturo Solares is a consultant for Medtronic. Gustavo Pradilla is a consultant for Stryker Corporation.
References
1. da Costa MD, Hardesty DA, Priddy B, Noiphithak R, Barbero JM, Prevedello DM. Extended supraorbital approach with modified eyebrow incision: Technical note. World Neurosurg. 2019. 128: 354-9
2. Louis DN, Perry A, Reifenberger G, von Deimling A, FigarellaBranger D, Cavenee WK. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016. 131: 803-20
3. Wilson DA, Duong H, Teo C, Kelly DF. The supraorbital endoscopic approach for tumors. World Neurosurg. 2014. 82: e243-56


James Ausman
Posted March 21, 2022, 8:31 pm
Excellent surgical technique and use of endoscope.