

- Department of Neurosurgery, Nanoori Gangnam Hospital, Seoul, South Korea
- Department of Spine Surgery, Sir Ganga Ram Hospital, New Delhi, India
- Medical School, University of Debrecen, Debrecen, Hungary
Correspondence Address:
Hyeun-Sung Kim
Department of Neurosurgery, Nanoori Gangnam Hospital, Seoul, South Korea
DOI:10.25259/SNI-175-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Hyeun-Sung Kim, Ravindra Singh, Nitin Adsul, Jung-Soo Bang, Chang-Hwang Park, Il-Tae Jang. Full endoscopic treatment of unusual spontaneous degenerative epidural cyst: A case report. 24-Apr-2019;10:58
How to cite this URL: Hyeun-Sung Kim, Ravindra Singh, Nitin Adsul, Jung-Soo Bang, Chang-Hwang Park, Il-Tae Jang. Full endoscopic treatment of unusual spontaneous degenerative epidural cyst: A case report. 24-Apr-2019;10:58. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=9299
Date of Submission
18-Oct-2018
Date of Acceptance
07-Mar-2019
Date of Web Publication
24-Apr-2019
Abstract
Background:Extensive studies have been performed about the synovial cyst and intraspinal extradural ganglion cyst. Here, we describe a new type of the cyst with entirely different histological characteristics, which we are now calling a “Spontaneous Degenerative Epidural Cyst.”
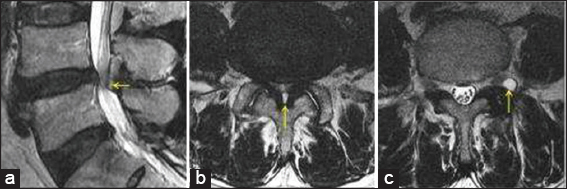
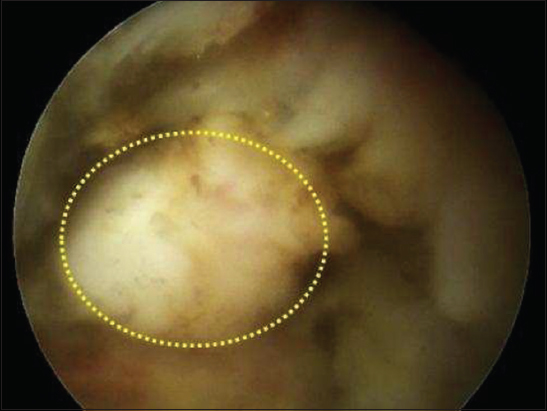
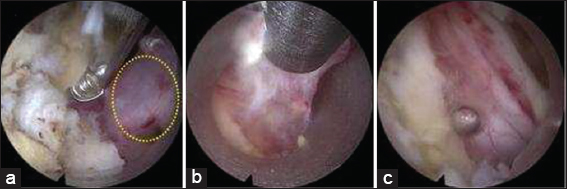
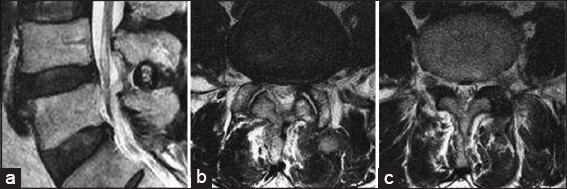
Case Description:A 74-year-old male presented with low back pain, bilateral lower extremity radiculopathy, and a cauda equina syndrome. He exhibited a partial left foot drop (Grade 3/5) and hypoesthesia in the sacral region. The magnetic resonance imaging (MRI) showed two cysts at the L4–L5 level; Cyst I was in the left foramen and Cyst II was within the epidural space between the dura and ligamentum flavum. Cyst I was removed through an endoscopic transforaminal approach; it originated from the left facet joint and with synovial lining was confirmed to be a synovial cyst. Cyst II required an endoscopic interlaminar approach, and pathology revealed granulation tissue with micro-calcification, woven bone formation, hemosiderin pigment, and focal cystic change consistent with our designation “Spontaneous Degenerative Epidural Cyst.”
Conclusion:“Spontaneous Degenerative Epidural cyst” should be considered among the differential diagnostic consideration for the different lumbar cysts. High-resolution MRI is the most useful in diagnosing these lesions, while full endoscopic treatment provides for adequate resection of these lesions.
Keywords: Endoscopic spine surgery, ganglion cyst, spontaneous degenerative epidural cyst, synovial cyst
INTRODUCTION
We have identified a unique type of intraspinal lumbar cyst, which we termed a “Spontaneous Degenerative Epidural Cyst,” located between the ligamentum flavum and dura. It was a distinctive feature since the connection was neither to the ligamentum flavum nor dura and it exhibited unique histological characteristics.
CASE REPORT
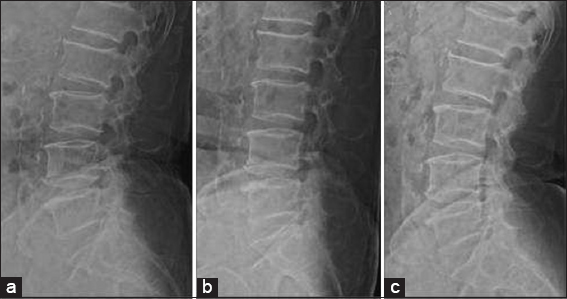
A 74-year-old male with 6-month history of lower extremity radiculopathy, acutely presented with a cauda equina syndrome. On examination, he had a left-sided partial foot drop (extensor hallucis longus dorsiflexion 3/5) and sacral hypoesthesia. The magnetic resonance (MR) imaging showed severe L4–L5 stenosis, and two lumbar cysts: cyst I was located in the left foramen, while Cyst II was situated between the dura and ligamentum flavum; there was no evidence of instability [Figures
Histology
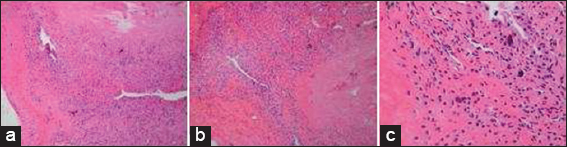
Cyst I originated from the facet joint and had a synovial lining consistent with a synovial cyst. The “Spontaneous Degenerative Epidural Cyst II,” located in the epidural space between the dura and the ligamentum flavum, showed granulation tissue with microcalcifications, woven bone formation, hemosiderin pigmentation, and focal cystic changes [
DISCUSSION
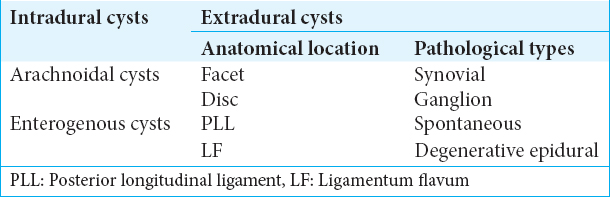
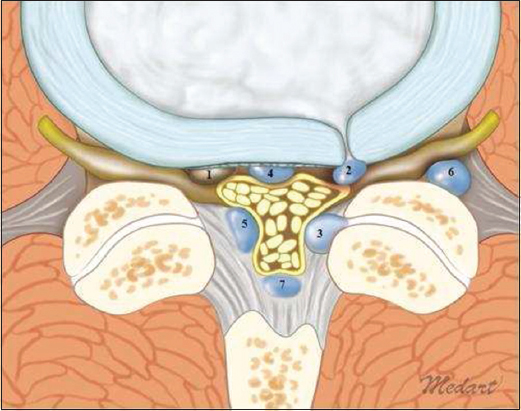
Lumbar intraspinal cysts can be either intradural or extradural [
In our patient with two cystic lesions, cyst I was a synovial cyst. Intraoperative and histological findings of cyst II did not, however, fit in the typical categories of synovial or ganglion cysts. Rather, cyst II with calcification, granulation tissue, and hemosiderin deposits reflected a degenerative process involving the central lumbar canal that we newly called a “Spontaneous Degenerative Epidural Cyst.”
CONCLUSION
Here, we report on a “Spontaneous Degenerative Epidural Cyst” involving the lumbar spinal canal. It should be considered among the differential diagnoses for lumbar cysts and is best diagnosed on MR. Full endoscopic resection provides symptomatic relief and pathological confirmation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. El Beltagi AH, Swamy N, Dashti F. Vacuum epidural cyst with acute neurological presentation. A case report. Neuroradiol J. 2013. 26: 213-7
2. Khalatbari K, Ansari H. MRI of degenerative cysts of the lumbar spine. Clin Radiol. 2008. 63: 322-8
3. Lake PA, Minckler J, Scanlan RL. Spinal epidural cyst:Theories of pathogenesis. Case report. J Neurosurg. 1974. 40: 774-8
4. Nojiri H, Sakuma Y, Uta S. Degenerative intraspinal cyst of the cervical spine. Orthop Rev (Pavia). 2009. 1: e17-

