

- Deparment of Neurosurgery, Juha Hernesniemi International Center, Henan Provincial People’s Hospital, University of Zhengzhou, Zhengzhou, China,
- Department of Neurosurgery, Yachiyo Medical Center, Tokyo Women’s Medical University, Chiba, Japan.
DOI:10.25259/SNI_460_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Jiangyu Xue, Hugo Andrade-Barazarte, Gangqin Xu, Dongyang Cai, Yang Bowen, Ajmal Zemmar, Juha Hernesniemi, Akitsugu Kawashima. Superficial temporal artery-superior cerebellar artery bypass and direct clipping of a large unruptured superior cerebellar artery aneurysm through subtemporal approach: Surgical video. 22-Nov-2019;10:225
How to cite this URL: Jiangyu Xue, Hugo Andrade-Barazarte, Gangqin Xu, Dongyang Cai, Yang Bowen, Ajmal Zemmar, Juha Hernesniemi, Akitsugu Kawashima. Superficial temporal artery-superior cerebellar artery bypass and direct clipping of a large unruptured superior cerebellar artery aneurysm through subtemporal approach: Surgical video. 22-Nov-2019;10:225. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=9769
Date of Submission
20-Aug-2019
Date of Acceptance
29-Oct-2019
Date of Web Publication
22-Nov-2019
Abstract
Background: Superior cerebellar artery (SCA) aneurysms are rare. Current treatments include: direct clipping, trapping ± bypass, and endovascular methods (coiling, stenting, or flow diversion). Due to specific characteristics (wide base, location, and shape), a major challenge while dealing with SCA aneurysms is to preserve the flow of the parent artery and perforators. This video demonstrates a revascularization procedure, and clip reconstruction of a large unruptured basilar artery (BA)/SCA aneurysm performed through the subtemporal approach.
Case Description: A 60-year-old woman presented with dizziness and headaches. Computed tomography angiography (CTA) and digital subtraction angiography showed a right unruptured large BA/SCA aneurysm. After multidisciplinary discussion, and considering gender, age, risk factors of the patient. Endovascular treatment was considered with a high risk of ischemic complications. Therefore, the patient was consented for a superficial temporal artery (STA)-SCA bypass through subtemporal approach followed by direct clipping/ trapping of the aneurysm. Postoperative CTA showed occlusion of the aneurysm and patency of the parent vessels. Postoperatively, the patient experienced immediate transient left mild monoparesis and right IV nerve palsy, which recovered completely at 6-months follow-up.
Results: Surgical treatment of SCA aneurysms is decreasing due to the existence of endovascular therapies such as stents and flow diverters. However, some cases may necessitate surgical treatment and revascularization procedures to maintain the blood flow of the parent artery and to treat the previous lesion.
Conclusion: The STA-SCA bypass through the subtemporal approach is a feasible option to maintain the blood flow of the parent artery in cases of SCA requiring surgical treatment and trapping/direct clipping of the aneurysm.
Keywords: Aneurysm, Bypass, Subtemporal approach, Superficial temporal artery/superior cerebellar artery
INTRODUCTION
Superior cerebellar artery (SCA) aneurysms are rare.[
CASE DESCRIPTION, (MULTIMEDIA 1) SURGICAL TECHNIQUE, AND OUTCOME
A 60-year-old right-handed woman presented with dizziness and headaches for approximately 2 months. Previous health history includes current smokers and hypertension. The patient underwent computed tomography angiography (CTA) and digital subtraction angiography (DSA) that showed a right unruptured SCA aneurysm measuring approximately 13 mm in maximum diameter and associated with bilateral hypoplastic P1 arteries. This aneurysm projected laterally had a wide base and it was highly positioned into the interpeduncular cistern. we offered treatment to this aneurysm, considering gender, age and risk factors of the patient (Hypertension and smoker). Endovascular treatment was considered with high risk of ischemic complications. Therefore, the patient was consented for a superficial temporal artery (STA)-SCA bypass through the subtemporal approach followed by aneurysm occlusion.
The patient is placed on the left side park-bench position. Then, a lumbar drainage is placed until obtain approximately 50–100 ml of cerebrospinal fluid (CSF) to decrease the risk of injuring the temporal lobe while mobilizing it. A straight skin incision followed the course of the parietal branch of the STA; then, it curved posteriorly above the earlobe. The main goal is to obtain approximately 7–8 cm of STA graft as donor graft. After dissecting the parietal branch of the STA, the temporal muscle is detached and retracted anteriorly and inferiorly until expose the root of the zygoma and the spine of Henle. A subtemporal craniotomy is performed, as described previously.[
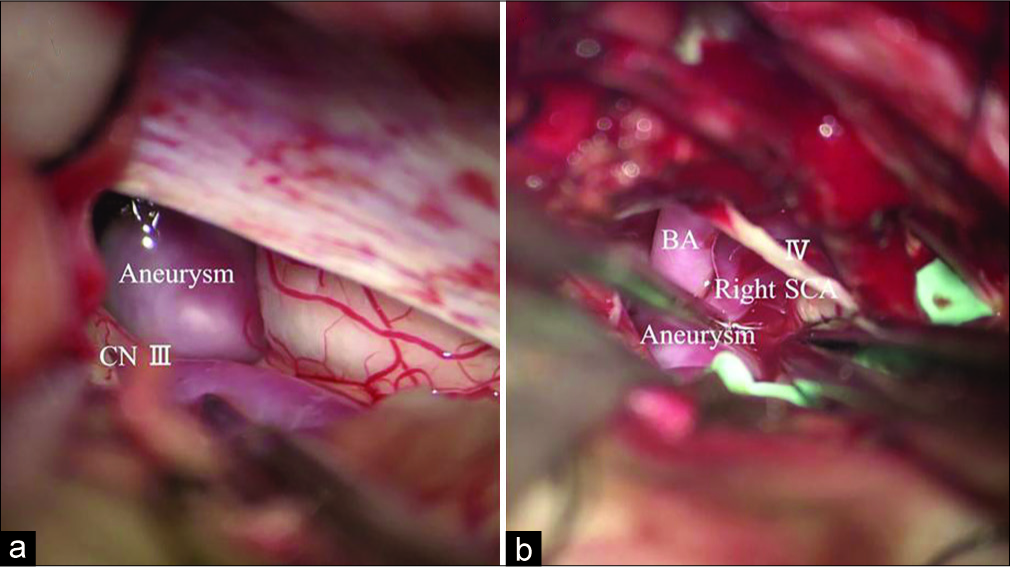
Therefore, after trying to re-shaping the aneurysm with bipolar coagulation, we proceed with direct clipping using two titanium clips. Indocyanine green video angiography was used to verify the patency of the bypass graft, perforators, and exclusion of the aneurysm.
Postoperative CTA showed occlusion of the aneurysm and patency of the parent vessels. Postoperatively, the patient experienced immediate transient left mild monoparesis and right IV nerve palsy; however, magnetic resonance imaging diffusion and perfusion images did not show any signs of ischemic event. At 6-months follow-up, the patient has no neurological deficit and the IV CN palsy recovered completely. DSA at 6-months showed patency of the STA- SCA bypass and aneurysm obliteration.
CONCLUSION
Microsurgical treatment of SCA aneurysms is decreasing due to the existence of endovascular therapies such as stents and flow diverters. However, some cases may necessitate surgical treatment and revascularization procedures to maintain the blood flow of the parent artery and to treat the previous lesion. The STA-SCA bypass through the subtemporal approach remains as a feasible option to maintain the blood flow of the parent artery in cases of SCA requiring surgical treatment and trapping/direct clipping of the aneurysm.
Multimedia 1: Clipping of a right unruptured superior cerebellar artery (SCA) aneurysm and superficial temporal artery to SCA bypass through the subtemporal approach
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos available on:
www.surgicalneurologyint.com
References
1. Briganti F, Marseglia M, Leone G, Briganti G, Piccolo D, Napoli M. Endovascular treatment of a small aneurysm of the superior cerebellar artery with a flow-diverter device. A case report. Neuroradiol J. 2013. 26: 327-31
2. Goehre F, Lehecka M, Jahromi BR, Lehto H, Kivisaari R, Hijazy F. Subtemporal approach to posterior cerebral artery aneurysms. World Neurosurg. 2015. 83: 842-51
3. Hayashi N, Kurimoto M, Nagai S, Sato H, Hori S, Endo S. Tentorial incision in a lateral-medial direction with minimal retraction of the temporal lobe in the subtemporal transtentorial approach to the middle tentorial incisural space. Minim Invasive Neurosurg. 2008. 51: 340-4
4. Jeon JB, Oh SY, Hyun DK, Shim YS. Fusiform superior cerebellar artery aneurysm treated with endovascular treatment. J Cerebrovasc Endovasc Neurosurg. 2016. 18: 276-80
5. Kang IH, Malla HP, Lee SH, Park CK, Choi SK. Revascularization as treatment of a ruptured fusiform aneurysm at the cortical segment of the superior cerebellar artery: A case report and literature review. J Neurol Surg A Cent Eur Neurosurg. 2017. 78: 302-5
6. Kawashima A, Andrade-Barazarte H, Jahromi BR, Oinas M, Elsharkawy A, Kivelev J. Superficial temporal artery: Distal posterior cerebral artery bypass through the subtemporal approach: Technical note and pilot surgical cases. Oper Neurosurg (Hagerstown). 2017. 13: 309-16
7. Peluso JP, van Rooij WJ, Sluzewski M, Beute GN. Superior cerebellar artery aneurysms: Incidence, clinical presentation and midterm outcome of endovascular treatment. Neuroradiology. 2007. 49: 747-51

