

- Department of Neurosurgery, Kanazawa University, Kanazawa, Ishikawa, Japan.
DOI:10.25259/SNI_432_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Katsuyoshi Miyashita, Ryouken Kimura, Sho Tamai, Shingo Tanaka, Masashi Kinoshita, Yasuhiko Hayashi, Mitsutoshi Nakada. Intratumoral continuous facial nerve stimulation for surgical resection of cystic vestibular schwannoma: Technical note. 29-Nov-2019;10:231
How to cite this URL: Katsuyoshi Miyashita, Ryouken Kimura, Sho Tamai, Shingo Tanaka, Masashi Kinoshita, Yasuhiko Hayashi, Mitsutoshi Nakada. Intratumoral continuous facial nerve stimulation for surgical resection of cystic vestibular schwannoma: Technical note. 29-Nov-2019;10:231. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=9777
Date of Submission
26-Jul-2019
Date of Acceptance
01-Nov-2019
Date of Web Publication
29-Nov-2019
Abstract
Background: Cystic vestibular schwannomas (CVSs) account for about 10% of VS. The efficacy of continuous facial nerve stimulation (CFS) was previously reported; however, it is often difficult to place the electrode at the root exit zone (REZ) in the early stage of surgical resection. We proposed a new method of intratumoral CFS (ICFS) by searching for the facial nerve through the cyst wall and leaving the spherically shaped electrode at this point.
Methods: The cyst wall was opened, and the ventral side of the tumor wall was stimulated to search for the positive point of facial nerve stimulation and place the spherically shaped electrode for continuous stimulation at this point through the cyst cavity (intensity: 0.2–1.5 mA, frequency: 1 Hz). Safe surgical resection could be performed under ICFS in all three cases.
Results: Good preservation of the facial nerve and extent of resection that was estimated preoperatively was achieved in all cases.
Conclusion: ICFS is suitable for the preservation of facial nerve function in surgical resection of CVS in cases in which electrode placement at the REZ is difficult.
Keywords: Cystic vestibular schwannoma, Intratumoral continuous facial nerve stimulation, Root exit zone
INTRODUCTION
Most vestibular schwannomas (VSs) are the solid type, and cystic VSs (CVSs) were reported to account for about 10% of VSs.[
MATERIALS AND METHODS
Three CVS patients underwent surgical resection with ICFS [

Anesthesia was maintained without muscle relaxants during microsurgery. A craniotomy and U-shaped dural incision were performed. We stimulated the dorsal side of the tumor wall with NIM after tumor exposure and dissected the tumor wall if there was no facial nerve function on the dorsal side. The tumor was resected through the cyst cavity, and NIM was used during tumor resection as required. If there was a positive response point on the ventral side of the tumor wall, a spherically shaped electrode was placed at the positive point. Stimulation strength was as low as possible, and the frequency of stimulation was 1 Hz during tumor resection. We often switched to occasional stimulation by NIM to identify the path of the facial nerve. If the amplitude was decreased, a medical technologist warned the surgeon immediately. We checked the appropriate initial placement of the electrode and paused tumor resection until recovery.
RESULTS
Case 1
An 84-year-old female who suffered from dizziness was referred to our hospital. Gadolinium (Gd)-contrast-enhanced magnetic resonance (MR) images showed cystic enhanced tumor 40 mm in diameter in the left cerebellopontine angle [CPA;
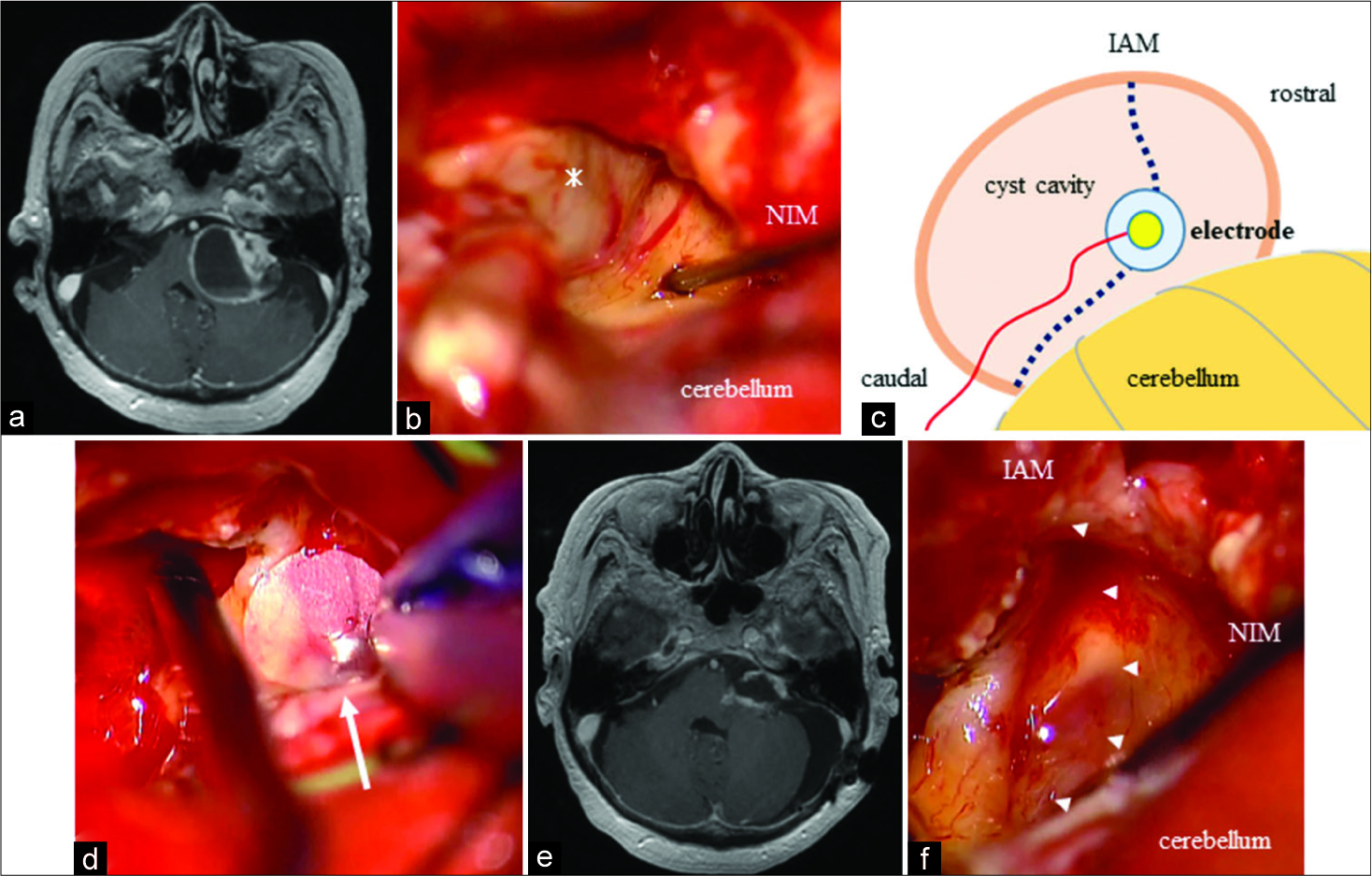
Figure 1:
Axial T1-weighted postcontrast magnetic resonance (MR) images and intraoperative scenes of case 1. Pre- (a) and post-operative (b) axial T1-weighted MR images showing subtotal cystic vestibular schwannomas resection with marked shrinkage. (c) Schematic of intratumoral continuous facial nerve stimulation (ICFS). Placement of the spherically shaped electrode at the ventral tumor wall through the tumor cavity at the positive point by occasional stimulation. Dotted line is the path of the facial nerve. (d) Positive point of ventral tumor wall stimulation by NIM through the cyst cavity (asterisk) after opening the cyst wall. (e) Positioning the spherically shaped electrode for ICFS (white arrow) at the positive point from c. (f) Estimated route of facial nerve, which responded positively to stimulation through the tumor wall (arrowheads). IAM: Internal auditory meatus.
Case 2
A 72-year-old male for whom a subtotal resection (STR) for a left CVS was performed 2 years prior. Two years after STR, he suffered from progressive left facial and abducens palsy. Gd- contrast-enhanced MR imaging showed cyst regrowth. We intended to achieve cyst shrinkage and perform postoperative stereotactic radiosurgery. Adhesion of the tumor wall to the surrounding structures was too tight to perform a dissection. The cyst wall was opened, and an electrode was placed at the NIM-positive point of ventral wall. The tumor was resected partially, and the cyst size was reduced [
Case 3
A 63-year-old female who suffered the right hearing disturbance presented at our department. MR images showed a right cystic enhanced lesion, and the brainstem and cerebellum were compressed. The facial nerve was identified through the cyst cavity at the ventrorostral side of the tumor cavity, and an electrode was placed. The electrode was replaced at the REZ of the facial nerve when REZ was visible after mass reduction. STR was achieved without facial nerve palsy [
DISCUSSION
The goal of VS surgical resection is maximal tumor resection and simultaneous preservation of facial nerve function. To preserve facial nerve function, two types of stimulation are used: occasional and continuous. When we use occasional facial nerve monitoring, it is difficult to recognize the facial nerve injury during the stimulation interval. CFS can monitor facial nerve injury immediately because the stimulation interval is just 1 s (1 Hz). The previous reports showed that the preservation ratio of facial nerve function was 98.6% with 98.2% tumor resection rate when using CFS.[
A suitable intensity for electrical stimulation of the facial nerve was reported. It is desirable that the intensity for exposed facial nerve stimulation is as low as possible (generally 0.1–0.2 mA).[
In a previous report of CVS, good facial nerve outcomes were achieved in 82% of STR or near-total resection patients, as compared with 73% of gross total resection patients.[
CONCLUSION
We presented the first report of ICFS for surgical resection of CVS. ICFS is suitable for surgical resection of CVS, in which leaving the electrode near the REZ is difficult.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Amano M, Kohno M, Nagata O, Taniguchi M, Sora S, Sato H. Intraoperative continuous monitoring of evoked facial nerve electromyograms in acoustic neuroma surgery. Acta Neurochir (Wien). 2011. 153: 1059-67
2. Eser Ocak P, Dogan I, Ocak U, Dinc C, Başkaya MK. Facial nerve outcome and extent of resection in cystic versus solid vestibular schwannomas in radiosurgery era. Neurosurg Focus. 2018. 44: E3-
3. Piccirillo E, Wiet MR, Flanagan S, Dispenza F, Giannuzzi A, Mancini F. Cystic vestibular schwannoma: Classification, management, and facial nerve outcomes. Otol Neurotol. 2009. 30: 826-34
4. Silverstein H, Rosenberg SI, Flanzer J, Seidman MD. Intraoperative facial nerve monitoring in acoustic neuroma surgery. Am J Otol. 1993. 14: 524-32
5. Sinha S, Sharma BS. Cystic acoustic neuromas: Surgical outcome in a series of 58 patients. J Clin Neurosci. 2008. 15: 511-5
6. Sobottka SB, Schackert G, May SA, Wiegleb M, Reiss G. Intraoperative facial nerve monitoring (IFNM) predicts facial nerve outcome after resection of vestibular schwannoma. Acta Neurochir (Wien). 1998. 140: 235-42
7. Yashar P, Zada G, Harris B, Giannotta SL. Extent of resection and early postoperative outcomes following removal of cystic vestibular schwannomas: Surgical experience over a decade and review of the literature. Neurosurg Focus. 2012. 33: E13-
8. Yokoyama T, Uemura K, Ryu H. Facial nerve monitoring by monopolar low constant current stimulation during acoustic neurinoma surgery. Surg Neurol. 1991. 36: 12-8

