

- Department of Psychiatry, Psychiatric Hospital of the University of Zürich, Militarstrasse, Zürich, Switzerland,
- Department of Neurosurgery, University Hospital of Liège, Avenue de L’hopital 1, Liège, Belgium.
- Department of Physical Therapy, University Hospital of Liège, Avenue de L’hopital 1, Liège, Belgium.
- Department of Medical Imaging, University Hospital of Liège, Avenue de L’hopital 1, Liège, Belgium.
- Department of Neuroanatomy, University Hospital of Liège, Avenue de L’hopital 1, Liège, Belgium.
Correspondence Address:
Felix Scholtes
Department of Neurosurgery, University Hospital of Liège, Avenue de L’hopital 1, Liège, Belgium.
Department of Neuroanatomy, University Hospital of Liège, Avenue de L’hopital 1, Liège, Belgium.
DOI:10.25259/SNI_351_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Werner Surbeck, Francois Gerardy, Aude Barjona Morgado De Moura, Louis Deprez, Didier Martin, Felix Scholtes. A case of aphasia due to temporobasal edema: Contemporary models of language anatomy are clinically relevant. 25-Jul-2020;11:212
How to cite this URL: Werner Surbeck, Francois Gerardy, Aude Barjona Morgado De Moura, Louis Deprez, Didier Martin, Felix Scholtes. A case of aphasia due to temporobasal edema: Contemporary models of language anatomy are clinically relevant. 25-Jul-2020;11:212. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10152
Date of Submission
13-Jun-2020
Date of Acceptance
20-Jun-2020
Date of Web Publication
25-Jul-2020
Abstract
Background: Understanding the anatomy of language in the human brain is crucial for neurosurgical decision making and complication avoidance. The traditional anatomical models of human language, relying on relatively simple and rigid concepts of brain connectivity, cannot explain all clinical observations. The clinical case reported here illustrates the relevance of more recent concepts of language networks involving white matter tracts and their connections.
Case Description: Postoperative edema of the ventral occipitotemporal cortex, where modern network models locate a crucial language hub, resulted in transient severe aphasia after a subtemporal approach. Both verbal comprehension and expression were lost. The resolution of edema was associated with complete recovery from phonetic and semantic dysfunction.
Conclusion: Complete aphasia due to a functional disturbance remote from the areas of Broca and Wernicke could be explained by contemporary neuroanatomical concepts of white matter connectivity. Knowledge of network-based models is relevant in brain surgery complication avoidance.
Keywords: Aphasia, Connectivity, Language, Networks, White matter tracts
BACKGROUND
The current understanding of language representation in the human brain has been reshaped by recent advances in brain imaging[
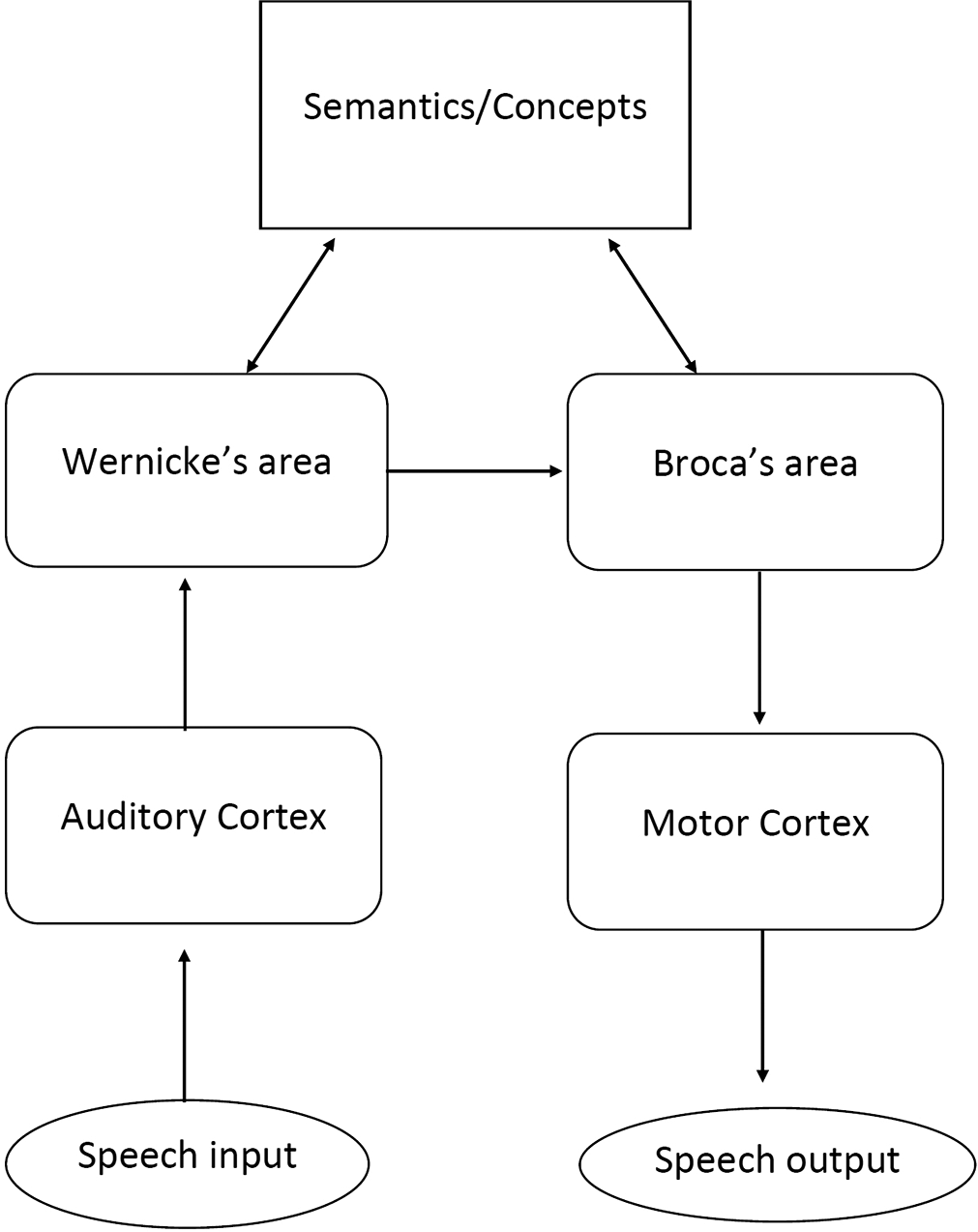
Figure 1:
The traditional Wernicke–Lichtheim model of language connectivity. The depicted connectivity permits serial, mainly unidirectional information processing. Semantic concepts are formed by higher associative systems distributed throughout the associative cortex, harboring conceptual representations of distinct modalities associated with a particular object.
Aphasia has been reported after subtemporal extra-axial approaches, without explanation of the underlying pathophysiology, besides possible vein of Labbé injury, or ill-defined temporal lobe edema mentioned in some cases.[
CASE DESCRIPTION
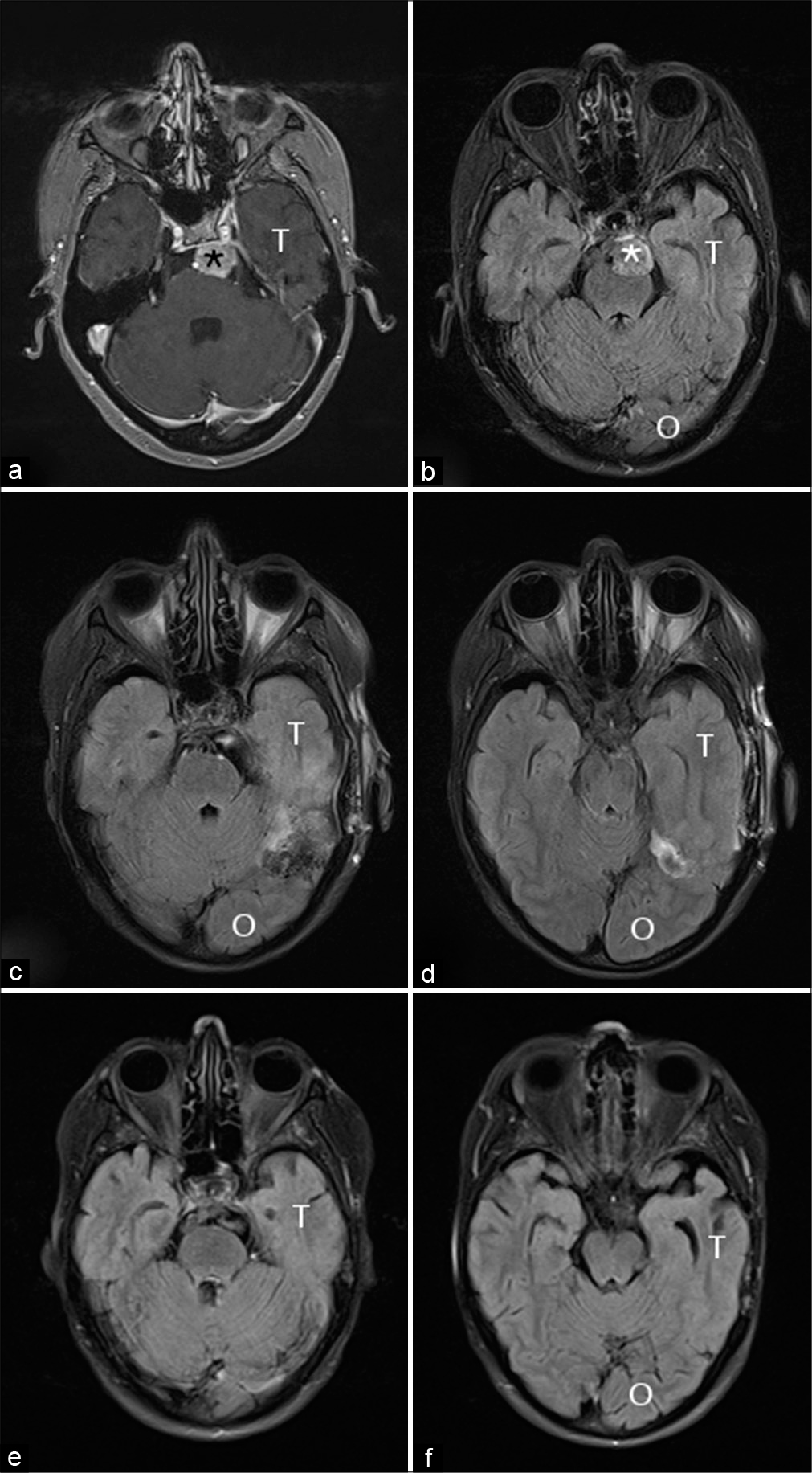
A 44-year-old woman with a history of whole-brain radiotherapy at age 9 for leukemia presented with slight dizziness. Left-sided headache was unchanged since childhood radiotherapy. Magnetic resonance imaging (MRI) showed three meningiomas, including one petroclival one showing growth at 1-year follow-up [
Immediate postoperative language function appeared normal. Over the first postoperative days, the patient developed progressive speech impairment, reaching mutism on the 2nd day. Five days after the operation, word-finding difficulties and deficient verbal comprehension persisted: the patient was incapable of naming objects or repeating sentences. Reading tests demonstrated verbal perseveration (VP).
Postoperative MRI 1 and 3 days after surgery showed an area of T2 hyperintensity at the inferior occipitotemporal junction [
Over the following days, language improved rapidly and, after 6 weeks, reading and comprehension had almost recovered: the semantic function was normal, phonemic fluency remained slightly deficient. At 1-year follow-up, these residual deficits resolved and language function completely returned to the preoperative state. MRI confirmed the expected resolution of the inferior temporal T2-hyperintensity. MRI diffusion tensor tractography was obtained 4 years after surgery to document the anatomy of white matter tracts involved in language. After the fusion of postoperative images and tractography, the lesion was located at the junction of the inferior longitudinal fasciculus (ILF), the inferior fronto-occipital fasciculus (IFOF) and the superior longitudinal fasciculus (SLF) [
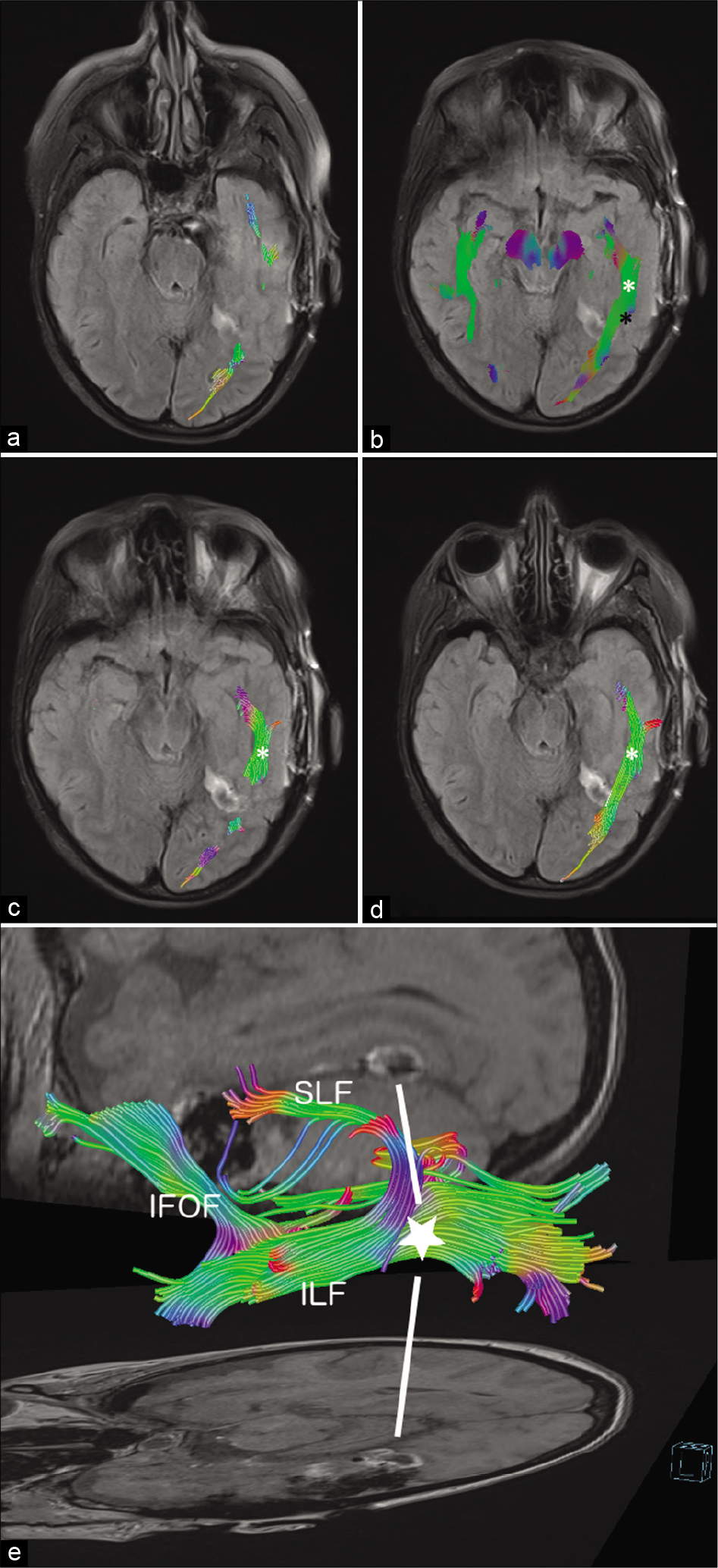
Figure 3:
Diffusion tensor imaging tractography 4 years after surgery, fused with initial 2D postoperative fluid-attenuated inversion recovery (FLAIR) magnetic resonance imaging (MRI) (syngo.via, Siemens, Munich, Germany). The ILF and inferior fronto-occipital fasciculus (IFOF) are part of the ventral stream and join posteriorly. The superior longitudinal fasciculus (SLF) represents the dorsal stream. (a-d): the reconstructed inferior longitudinal fasciculus (ILF) (white asterisk and green fibers) and posterior part of the IFOF, including their junction with the SLF (black asterisk and blue fibers), are depicted on craniocaudal axial FLAIR slices in relation to the temporobasal hypersignal. (e): 3D VRT reconstruction of the SLF, IFOF, and ILF in relation to the temporal FLAIR hypersignal (white star and lines, at the junction of the three tracts) on axial and sagittal images.
DISCUSSION
In the described case, severe mixed aphasia reaching mutism was attributable to a transient functional disturbance at the ventral temporooccipital junction. This area is located remote from the components of the classical Wernicke–Lichtheim model of language connectivity: the “language areas” of Broca and Wernicke and their direct connection through the arcuate fasciculus.[
Network concepts, more than unidirectional information processing, can provide satisfactory models for brain function. In short, parallel and bidirectional white matter connections of functionally related cortical areas (so-called “edges”) provide the anatomical basis for integrative processes and dynamic interactions. Critical cortical epicenters (so-called “hubs”) integrate plurimodal information originating in unimodal regions.[
White matter tracts have traditionally been investigated through postmortem gross dissection, fiber tract-tracing in animals, human functional imaging, and in vivo mapping by diffusion tensor imaging.[
According to this concept, language processing can be explained by a dual-stream architecture analogous to that of the visual system.[
Finally, parallel pathways of one stream may be, at least partially, functionally redundant. This provides an explanation, for example, for the well-known tolerance of anterior temporal lobectomy in the “dominant” hemisphere. The surgically inevitable loss of the indirect bundle (ILF-UF) of the ventral stream may, at least partly, clinically be compensated for by the direct pathway (IFOF),[
At the cortex of the ventral occipitotemporal junction, the dorsal stream (SLF) connects with both bundles of the ventral stream (ILF and IFOF) [
In summary, the function of the ventral occipitotemporal cortex as a crucial hub in current neuroanatomical language models explained complete transient aphasia with loss of both verbal comprehension and expression. Phonological, articulatory, and semantic function recovered with the resolution of occipitotemporal edema.
CONCLUSION
The present case of a complete loss of speech function could be satisfactorily explained by contemporary neuroanatomical concepts of white matter connectivity. Knowledge of network-based models is clinically relevant in brain surgery complication avoidance.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Axer H, Klingner CM, Prescher A. Fiber anatomy of dorsal and ventral language streams. Brain Lang. 2013. 127: 192-204
2. Catani M, Jones DK, Ffytche DH. Perisylvian language networks of the human brain. Ann Neurol. 2005. 57: 8-16
3. Catani M, Schotten MT. A diffusion tensor imaging tractography atlas for virtual in vivo dissections. Cortex. 2008. 44: 1105-32
4. Chen LF, Yu XG, Bu B, Xu BN, Zhou DB. The retrosigmoid approach to petroclival meningioma surgery. J Clin Neurosci. 2011. 18: 1656-61
5. Chen Y, Huang L, Chen K, Ding J, Zhang Y, Yang Q. White matter basis for the hub-and-spoke semantic representation: Evidence from semantic dementia. Brain. 2020. 143: 1206-19
6. Duffau H, Moritz-Gasser S, Mandonnet E. A Re-examination of neural basis of language processing: Proposal of a dynamic hodotopical model from data provided by brain stimulation mapping during picture naming. Brain Lang. 2014. 131: 1-10
7. Duffau H, Herbet G, Moritz-Gasser S. Toward a pluri-component, multimodal, and dynamic organization of the ventral semantic stream in humans: Lessons from stimulation mapping in-awake patients. Front Syst Neurosci. 2013. 7: 44-
8. Eguchi T, Fuchinoue T, Yahagi Y. Posterior subtemporal transtentorial approach for a lower basilar trunk aneurysm (author’s transl). No Shinkei Geka. 1979. 7: 513-7
9. Ercan S, Scerrati A, Wu P, Zhang J, Ammirati M. Is less always better? Keyhole and standard subtemporal approaches: Evaluation of temporal lobe retraction and surgical volume with and without zygomatic osteotomy in a cadaveric model. J Neurosurg. 2017. 127: 157-64
10. Hagner M, Hagner M, Rheinberger HJ, Wahrig-Schmidt B.editors. Lokalisation, funktion, cytoarchitektonik: Wege zur modellierung des gehirns. Objekte, Differenzen, Konjunkturen. Experimentalsysteme Im Historischen Kontext. Berlin: Akademie Verlag; 1994. p. 121-50
11. Hickok G, Poeppel D. Dorsal and ventral streams: A framework for understanding aspects of the functional anatomy of language. Cognition. 2004. 92: 67-99
12. Hickok G, Poeppel D. The cortical organization of speech processing. Nat Rev Neurosci. 2007. 8: 393-402
13. Ius T, Angelini E, Schotten MT, Mandonnet E, Duffau H. Evidence for potentials and limitations of brain plasticity using an atlas of functional resectability of WHO Grade II gliomas: Towards a minimal common brain. Neuroimage. 2011. 56: 992-1000
14. Khan OH, Herbet G, Moritz-Gasser S, Duffau H. The role of left inferior fronto-occipital fascicle in verbal perseveration: A brain electrostimulation mapping study. Brain Topogr. 2014. 27: 403-11
15. Martino J, Brogna C, Robles SG, Vergani F, Duffau H. Anatomic dissection of the inferior fronto-occipital fasciculus revisited in the lights of brain stimulation data. Cortex. 2010. 46: 691-9
16. Sabatino G, Rigante L, Marchese E, Albanese A, Esposito G, Capone G. Anterior subtemporal approach for posterolateral brainstem cavernomas: Report of ten cases. Acta Neurochir (Wien). 2012. 154: 2009-16
17. Saur D, Kreher BW, Schnell S, Kümmerer D, Kellmeyer P, Vry MS. Ventral and dorsal pathways for language. Proc Natl Acad Sci USA. 2008. 105: 18035-40
18. Surbeck W, Hänggi J, Scholtes F, Viher PV, Schmidt A, Stegmayer K. Anatomical integrity within the inferior fronto-occipital fasciculus and semantic processing deficits in schizophrenia spectrum disorders. Schizophr Res. 2020. 218: 267-75
19. Surbeck W, Hildebrandt G, Duffau H. The evolution of brain surgery on awake patients. Acta Neurochir (Wien). 2015. 157: 77-84
20. Ungerleider LG, Haxby JV. What’ and where in the human brain. Curr Opin Neurobiol. 1994. 4: 157-65
21. van den Heuvel MP, Sporns O. Network hubs in the human brain. Trends Cogn Sci. 2013. 17: 683-96
22. Vigneau M, Beaucousin V, Hervé PY, Duffau H, Crivello F, Houdé O. Meta-analyzing left hemisphere language areas: Phonology, semantics, and sentence processing. Neuroimage. 2006. 30: 1414-32
23. Wernicke C.editors. Der Aphasische Symptomencomplex, Eine Psychologische Studie auf Anatomischer Basis. Breslau: M. Cohn und Weigert; 1874. p.
24. Xu Z, ZEng X, Tian D, Chen Q. Microsurgical resection of petroclival tumors via the subtemporal transtentorial approach. Turk Neurosurg. 2016. 26: 331-5
25. Yang J, Liu YH, Ma SC, Wei L, Lin RS, Qi JF. Subtemporal transtentorial petrosalapex approach for giant petroclival meningiomas: Analyzation and evaluation of the clinical application. J Neurol Surg B Skull Base. 2012. 73: 54-63
26. Yeatman JD, Rauschecker AM, Wandell BA. Anatomy of the visual word form area: Adjacent cortical circuits and long-range white matter connections. Brain Lang. 2013. 125: 146-55

