

- Department of Neurosurgery, Kagawa Rosai Hospital, Kagawa, Japan
Correspondence Address:
Masatoshi Yunoki
Department of Neurosurgery, Kagawa Rosai Hospital, Kagawa, Japan
DOI:10.4103/2152-7806.159378
Copyright: © 2015 Yunoki M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Yunoki M, Suzuki K, Uneda A, Yoshino K. A case of dumbbell-shaped epidural cavernous angioma in the lumbar spine. Surg Neurol Int 25-Jun-2015;6:
How to cite this URL: Yunoki M, Suzuki K, Uneda A, Yoshino K. A case of dumbbell-shaped epidural cavernous angioma in the lumbar spine. Surg Neurol Int 25-Jun-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/a-case-of-dumbbell%e2%80%91shaped-epidural-cavernous-angioma-in-the-lumbar-spine/
Abstract
Background:Most spinal cavernous haemangiomas occur in the vertebral body and purely extradural cavernous hemangiomas without any vertebral body involvement is rare and account for only 4% of all extradural spinal tumors. Dumbbell-shaped spinal cavernous angioma is extremely rare, only 10 cases have been reported in the literature.
Case Description:A 77-year-old female presented with a one-year history of lumbago and right-sided L3 dermatomal hypoesthesia. A dumbbell mass at the L2/3 vertebral level was identified on lumbar MRI. The lesion was irregularly shaped and isointense on T1W and hyperintense on T2W and DWI images with homogenous contrast enhancement. A presumptive diagnosis was schwannoma, but other malignant neoplasms were also considered because of its irregular shape, minimally dilated neural foramen and the involvement of the non-enhanced L3 nerve root. The patient underwent surgery with a lateral extracavitary approach. A histopathological examination revealed cavernous hemangioma.
Conclusion:Cavernous hemangioma should be included in the differential diagnosis of dumbbell-shaped spinal tumors when the intervertebral foramina is not highly dilated and non-enhanced nerve root is identified in the tumor.
Keywords: Cavernous hemangioma, differential diagnosis, dumbbell, epidural, lumbar
INTRODUCTION
Most spinal cavernous hemangiomas occur in the vertebral body and may sometimes extend into the epidural space.[
CASE REPORT
A 77-year-old female presented with a 1-year history of lumbago and right-sided L3 dermatomal hypoesthesia. Her muscle strength and deep tendon reflexes were normal. Magnetic resonance imaging (MRI) of the lumbar spine revealed an irregularly-shaped, well-circumscribed paraspinal mass with minor intraspinal extension through the L2/3 intervertebral foramen. The lesion was isointense on T1-weighted (T1W) and hyperintense on T2W and diffusion-weighted images, with strong homogenous enhancement in a gadolinium (Gd) contrast study [
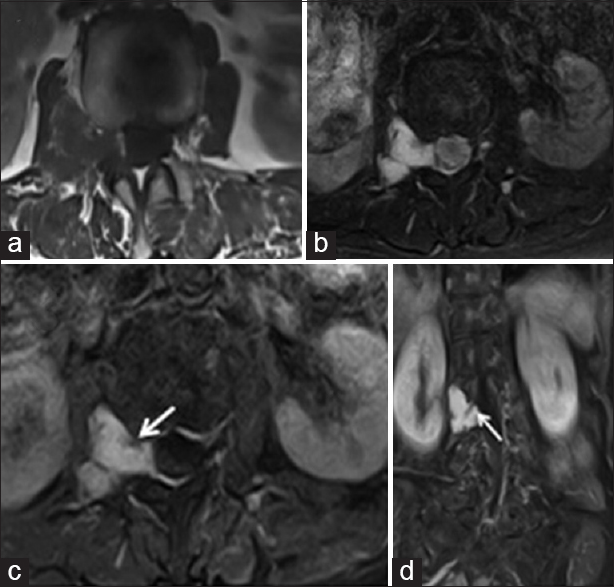
Figure 1
Preoperative magnetic resonance images at the level of L2/3 showing an irregularly-shaped, well-defined extradural lesion with paraspinal transforaminal extension that was hypointense on T1-weighted (T1W) (a) and hyperintense on T2W (b) and diffusion-weighted images. (c) Contrast-enhanced T1W images of transverse (d) and coronal sections showed the right L3 nerve root ventrally separated from the homogeneously enhanced tumor (arrow)
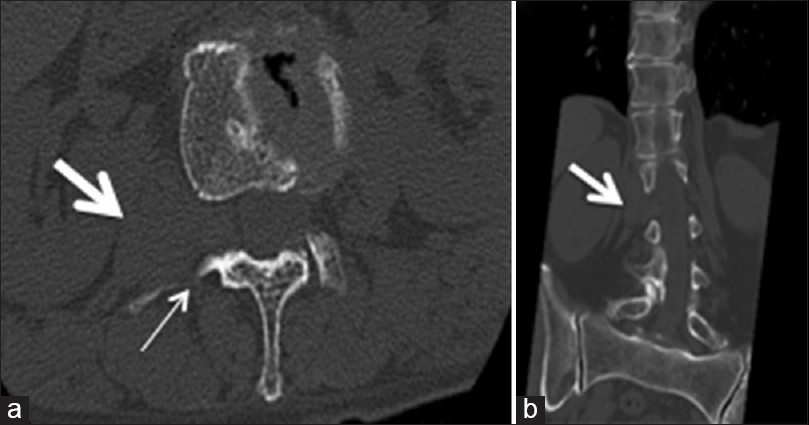
Figure 2
(a) A transverse computed tomography (CT) scan at the level of L2/3 showing a left-sided dumbbell-shaped mass (thick arrow). The posterior wall of the right intervertebral foramen was slightly eroded (thin arrow). (b) A coronal CT scan demonstrating the mildly enlarged right intervertebral foramen and dumbbell-shaped mass (thick arrow)
A longitudinal right paravertebral skin incision 15 cm in length at the L1–L3 level was made, followed by clear identification of the lumbodorsal fascia. The fascia was then incised in line, and a clear plane was identified between the multifidus medially and the longissimus laterally. The muscles were meticulously teased apart. The transverse processes of Th2 and Th3 were identified by fluoroscopy [
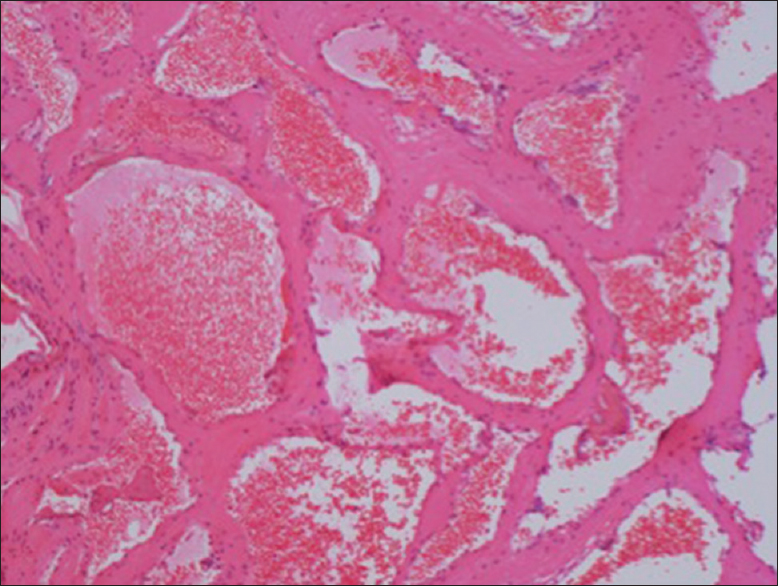
Figure 3
A microscopic examination revealed numerous dilated vascular channels of variable sizes lined by a single layer of flattened epithelial cells that was filled with blood elements. The tumor stroma consisted of typical fibrous tissue. The histological findings were characteristic of cavernous hemangioma. (H and E, ×100)
DISCUSSION
Hemangiomas are congenital vascular malformations whose pathologies are considered to be hamartomatous malformations.[
About 80% of spinal epidural cavernous angiomas are in the thoracic spine, most of which are located posterior within the spinal canal and present with myelopathy.[
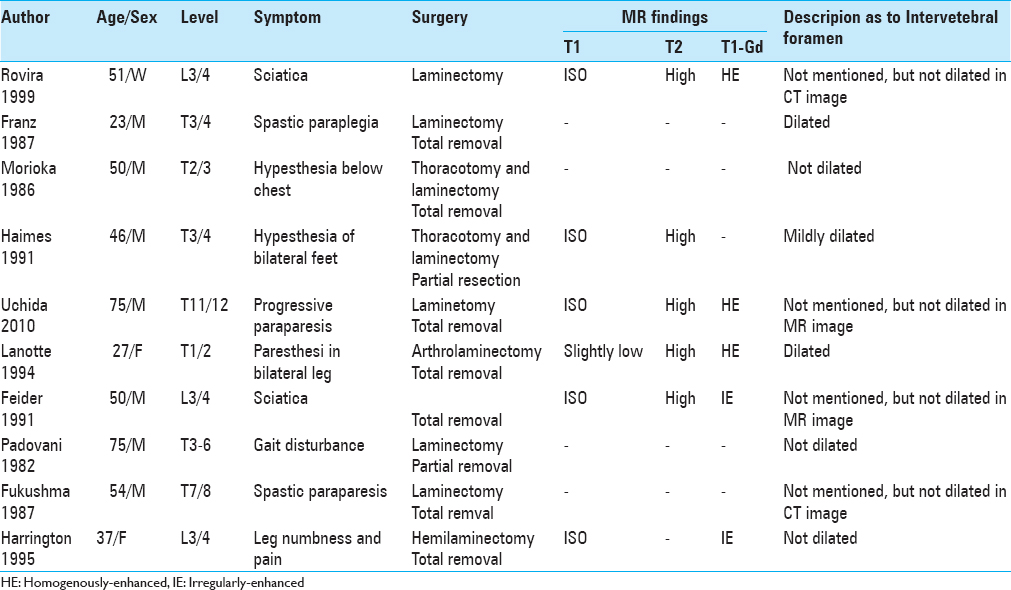
Dumbbell-shaped spinal tumors are usually thought to be schwannomas, neurofibromas or meningiomas.[
It has been suggested that a complete excision of the cavernous angioma is related to a favorable outcome. In the present case, however, we left a small amount of the tumor around the nerve root behind due to concerns about possible nerve root damage. When complete removal is not possible, radiosurgery is increasingly becoming an option, as advances in radiosurgical equipment are enabling safe and accurate targeting of lesions.[
References
1. Acciarri N, Padovani R, Giulioni M, Gaist G. Surgical treatment of spinal cavernous angiomas. J Neurosurg Sci. 1993. 37: 209-15
2. Aoyagi N, Kojima K, Kasai H. Review of spinal epidural cavernous hemangioma. Neurol Med Chir (Tokyo). 2003. 43: 471-5
3. Feider HK, Yuille DL. An epidural cavernous hemangioma of the spine. AJNR Am J Neuroradiol. 1991. 12: 243-4
4. Fontaine S, Melanson D, Cosgrove R, Bertrand G. Cavernous hemangiomas of the spinal cord: MR imaging. Radiology. 1988. 166: 839-41
5. Franz K, Lesoin F, Leys D, Krivosic I, Jomin M. Spinal epidural dumbbell-shaped cavernous angioma. Rev Neurol (Paris). 1987. 143: 298-300
6. Fukushima M, Nabeshima Y, Shimazaki K, Hirohata K. Dumbbell-shaped spinal extradural hemangioma. Arch Orthop Trauma Surg. 1987. 106: 394-6
7. Guthkelch AN. Haemangiomas involving the spinal epidural space. J Neurol Neurosurg Psychiatry. 1948. 11: 199-210
8. Haimes AB, Krol G. Dumbbell-shaped spinal cavernous hemangioma: A case report. AJNR Am J Neuroradiol. 1991. 12: 1021-2
9. Harrington JF, Khan A, Grunnet M. Spinal epidural cavernous angioma presenting as a lumbar radiculopathy with analysis of magnetic resonance imaging characteristics: Case report. Neurosurgery. 1995. 36: 581-4
10. Isoda H, Takahashi M, Mochizuki T, Ramsey RG, Masui T, Takehara Y. MRI of dumbbell-shaped spinal tumors. J Comput Assist Tomogr. 1996. 20: 573-82
11. Lanotte M, Massaro F, Faccani G, Forni M, Valentini MC. Dumbbell-shaped spinal epidural cavernous angioma. Case report. Ital J Neurol Sci. 1994. 15: 429-32
12. Morioka T, Nakagaki H, Matsushima T, Hasuo K. Dumbbell-shaped spinal epidural cavernous angioma. Surg Neurol. 1986. 25: 142-4
13. Padolecchia R, Acerbi G, Puglioli M, Collavoli PL, Ravelli V, Caciagli P. Epidural spinal cavernous hemangioma. Spine (Phila Pa 1976). 1998. 23: 1136-40
14. Padovani R, Tognetti F, Proietti D, Pozzati E, Servadei F. Extrathecal cavernous hemangioma. Surg Neurol. 1982. 18: 463-5
15. Rovira A, Rovira A, Capellades J, Zauner M, Bella R, Rovira M. Lumbar extradural hemangiomas: Report of three cases. AJNR Am J Neuroradiol. 1999. 20: 27-31
16. Sohn MJ, Lee DJ, Jeon SR, Khang SK. Spinal radiosurgical treatment for thoracic epidural cavernous hemangioma presenting as radiculomyelopathy: Technical case report. Neurosurgery. 2009. 64: E1202-3
17. Uchida K, Yayama T, Nakajima H, Hirai T, Kobayashi S, Chen K. Microsurgical resection of cavernous haemangioma around the thoracic neuroforamen: A case report. J Orthop Surg (Hong Kong). 2010. 18: 370-3
18. Wiltse LL, Bateman JG, Hutchinson RH, Nelson WE. The paraspinal sacrospinalis-splitting approach to the lumbar spine. J Bone Joint Surg Am. 1968. 50: 919-26

