

- Department of Neurosurgery, University of Texas Health Science Center, San Antonio, Texas, United States.
- Department of Pathology, University of Texas Health Science Center, San Antonio, Texas, United States.
Correspondence Address:
Uma Gonchigar, Department of Neurosurgery, University of Texas Health Science Center at San Antonio, San Antonio, United States.
DOI:10.25259/SNI_1171_2022
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Uma Gonchigar1, Taryn Cazzolli2, Samon Tavakoli-Sabour1, Viktor Bartanusz1. A lumbar chondroma originating from the intervertebral disc. 24-Feb-2023;14:67
How to cite this URL: Uma Gonchigar1, Taryn Cazzolli2, Samon Tavakoli-Sabour1, Viktor Bartanusz1. A lumbar chondroma originating from the intervertebral disc. 24-Feb-2023;14:67. Available from: https://surgicalneurologyint.com/surgicalint-articles/12170/
Date of Submission
30-Dec-2022
Date of Acceptance
07-Feb-2023
Date of Web Publication
24-Feb-2023
Abstract
Background: Chondromas, benign cartilaginous primary bone tumors, seldom occur in the spine. Most spinal chondromas arise from the cartilaginous parts of the vertebra. Chondromas originating from the intervertebral disc are extraordinarily rare.
Case Description: A 65-year-old female experienced recurrence of low back pain and left-sided lumbar radiculopathy after microdiscectomy and microdecompression. A mass continuous with the intervertebral disc was found to be compressing the left L3 nerve root and was resected. Histologic examination revealed a benign chondroma.
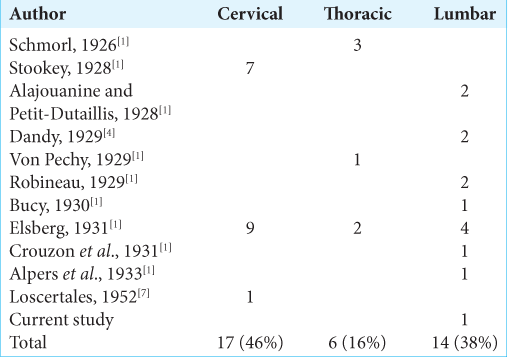
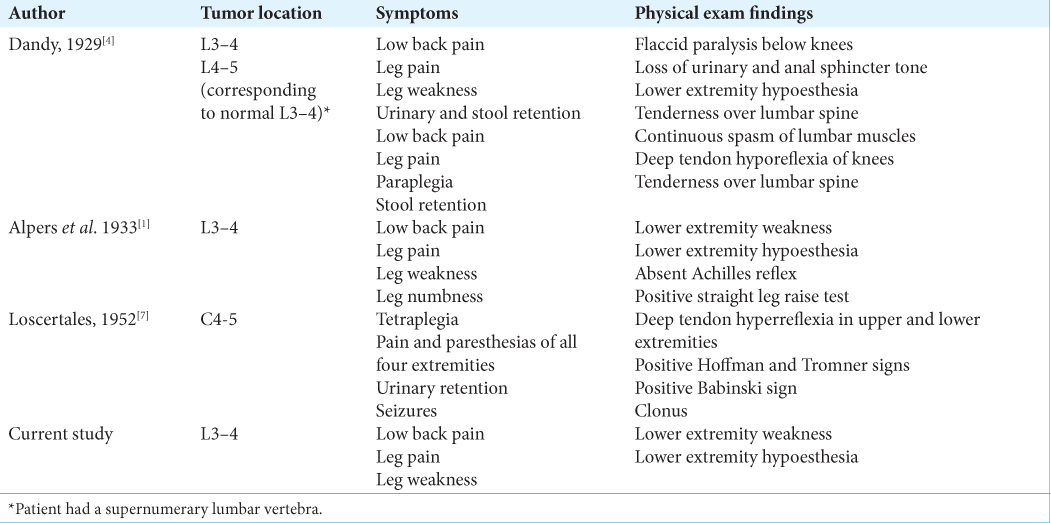
Conclusion: Chondromas developing from the intervertebral disc are extremely rare; we could find only 37 reported cases. Identification of these chondromas is difficult because until surgical resection they are almost indistinguishable from herniated intervertebral discs. Here, we describe a patient with residual/recurrent lumbar radiculopathy caused by a chondroma originating from the L3–4 intervertebral disc. When a patient has recurrence of spinal nerve root compression after discectomy, a chondroma arising from the intervertebral disc is an uncommon but possible etiology.
Keywords: Chondroma, Extraforaminal disc herniation, Nerve sheath tumor, Spinal tumor
INTRODUCTION
Chondromas are benign tumors composed of cartilage. Chondromas of the spine are uncommon, comprising 2% of spinal tumors, and most reported cases are in the cervical spine.[
CASE PRESENTATION
A 65-year-old female presented with 3 months of low back pain and left hip pain. Magnetic resonance imaging (MRI) revealed a cystic-appearing lesion in the left L3–4 neural foramen, thought to be a left-sided extraforaminal disc herniation [
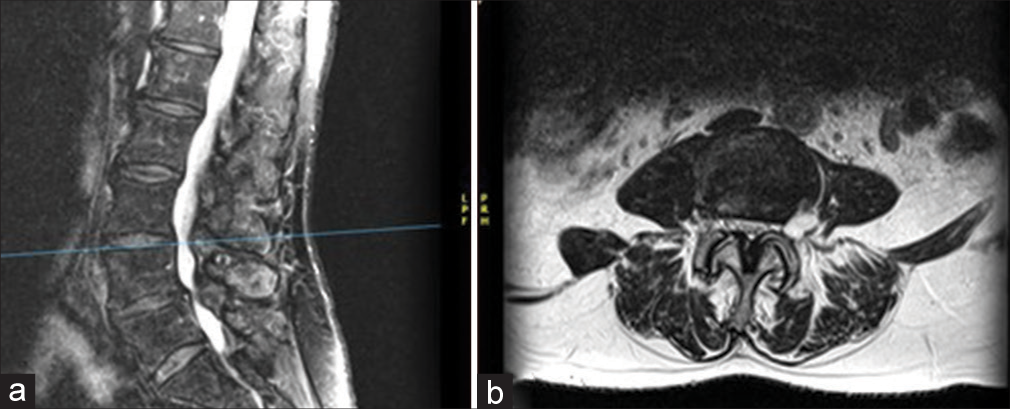
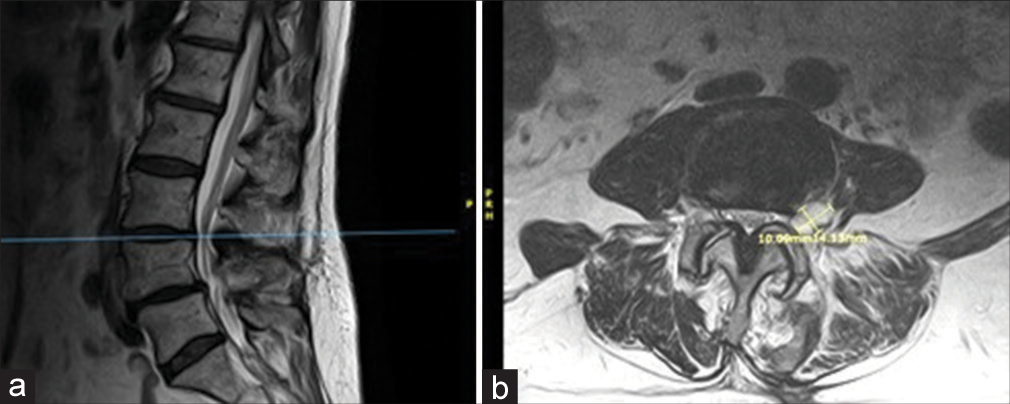
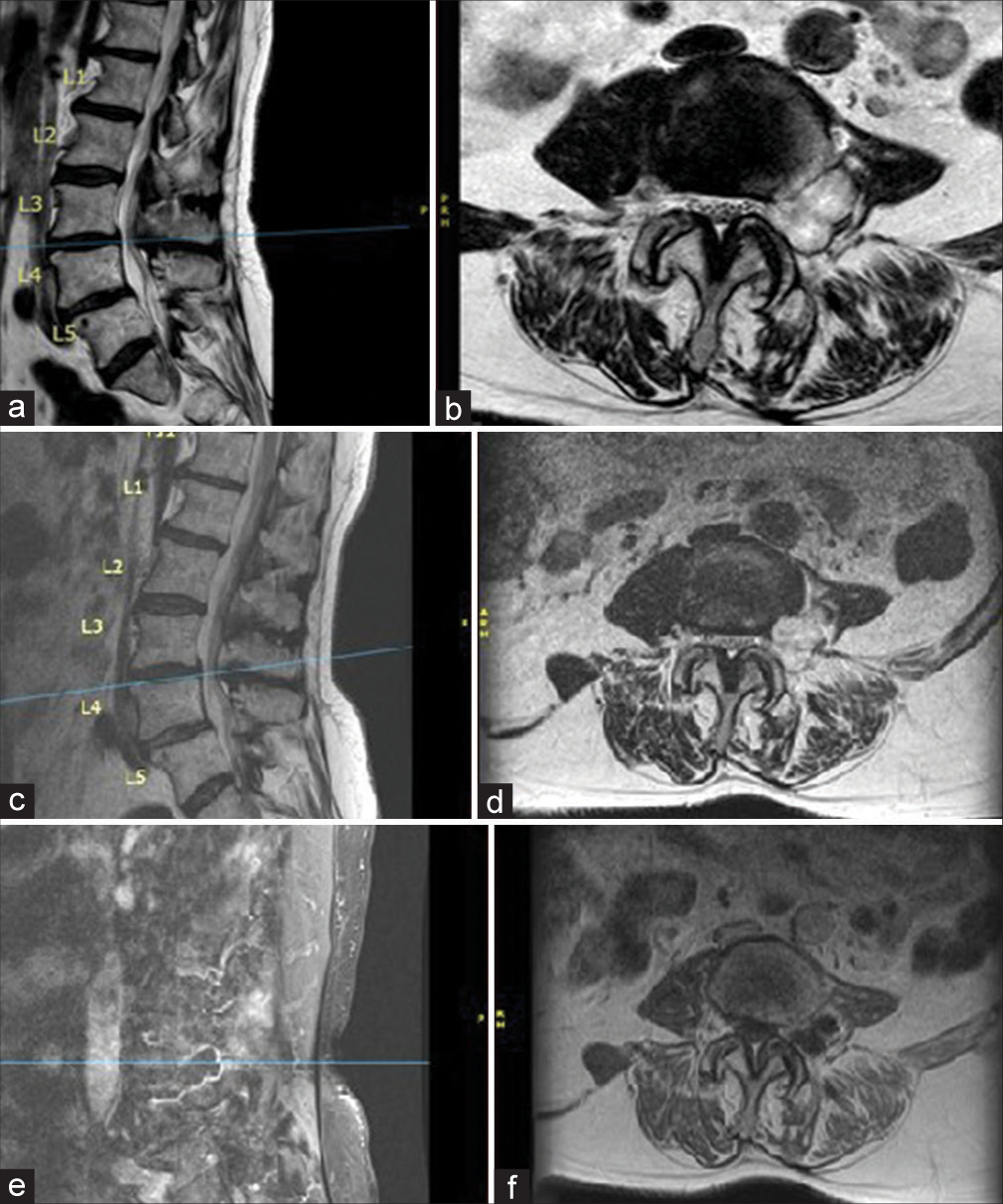
Figure 3:
Preoperative magnetic resonance imaging before second surgery. (a) T2 parasagittal without contrast. Progressive enlargement of lesion in the left L3–4 neural foramen with marked mass effect on the exiting L3 nerve visible on (b) T2 axial without contrast at L3–4. (c) T2 parasagittal without contrast. Redemonstration of lobulated T2-hyperintense mass measuring 2.5 × 2.4 × 2 cm centered in the left neural foramen visible on (d) T2 axial without contrast at L3–4. Peripherally enhancing cystic mass visible on (e) T1 parasagittal with contrast and (f) T1 axial with contrast at L3–4.
Pathology
Grossly, the tumor was lobulated and contained well-formed hyaline cartilage. Microscopically, it was a cartilaginous neoplasm with mild atypia but without mitoses or any myxoid areas. These findings were consistent with a benign extraosseous chondroid lesion, most likely chondroma versus chondromatosis [
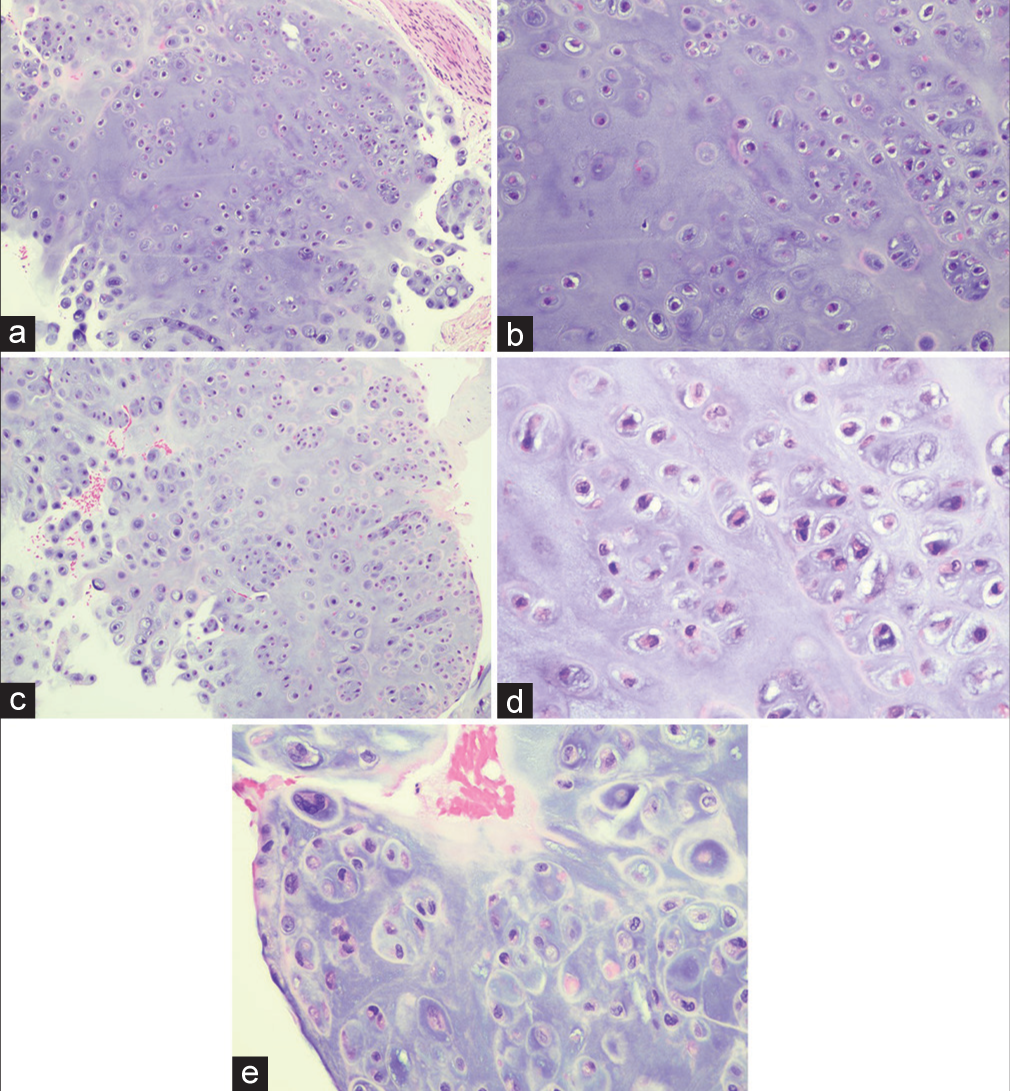
Figure 4:
Hematoxylin and eosin staining of the specimen. (a and b) Cellularity is somewhat increased compared to normal cartilage, but there is only mild atypia, no mitoses, and no myxoid areas. (c) Lobulated architecture of the cartilaginous neoplasm. (d) Bland histologic features, no atypia, no mitoses, favoring a benign extraosseous chondroid lesion. (e) A rare focus of mild atypia in the otherwise histologically bland neoplasm.
One-year follow-up
Within the next year, despite four postoperative MRI scans showing no new mass, no abnormal enhancement, and no significant change in the resection cavity, the patient still experienced residual weakness but had improved left leg pain.
DISCUSSION
Chondromas are benign, cartilaginous primary bone tumors, most commonly found in the small bones of the hands and feet. Only 2% occur in the spine.[
CONCLUSION
This case illustrates that when a patient experiences recurrent pain, weakness, and a MRI-documented recurrent mass following a prior discectomy, one should consider a possible underlying chondroma.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Alpers BJ, Grant FC, Yaskin JC. Chondroma of the intervertebral disks. Ann Surg. 1933. 97: 10-8
2. Bland LI, McDonald JV. Chondroma of the lumbar spine, a rare cause of sciatica: Case report. Neurosurgery. 1990. 26: 685-7 discussion 688
3. Dahlin DC, Unni KK, editors. Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases. Philadelphia, PA: Lippincott-Raven; 1996. p. 463
4. Dandy WE. Loose cartilage from intervertebral disk simulating tumor of the spinal cord By Walter E Dandy, 1929. Clin Orthop Relat Res. 1989. 238: 4-8
5. Elsberg CA, editors. Tumors of the Spinal Cord. New York: P.B. Hoeber; 1925. p.
6. Kim DH, Nam KH, Choi BK, Han I. Lumbar spinal chondroma presenting with acute sciatica. Korean J Spine. 2013. 10: 252-4
7. Loscertales F. Intraspinal cervical chondroma, probable discal origin, associated with tetraplegia. Acta Neurochir (Wien). 1952. 3: 93-9
8. McLoughlin GS, Sciubba DM, Wolinsky JP. Chondroma/ chondrosarcoma of the spine. Neurosurg Clin N Am. 2008. 19: 57-63
9. Robles LA, Mundis GM. Chondromas of the lumbar spine: A systematic review. Global Spine J. 2021. 11: 232-9
10. Slowik T, Bittner-Manioka M, Grochowski W. Case reports and technical notes. Chondroma of the cervical spine. Case report. J Neurosurg. 1968. 29: 276-9

