

- Department of Neurosurgery, Avicenne Military Hospital of Marrakech, Mohammed V University in Rabat, Rabat, Morocco
Correspondence Address:
Ali Akhaddar
Department of Neurosurgery, Avicenne Military Hospital of Marrakech, Mohammed V University in Rabat, Rabat, Morocco
DOI:10.4103/sni.sni_89_18
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Ali Akhaddar, Mohamed Boucetta. A new surgical technique for the removal of extensive spinal epidural hydatid cyst. 07-May-2018;9:96
How to cite this URL: Ali Akhaddar, Mohamed Boucetta. A new surgical technique for the removal of extensive spinal epidural hydatid cyst. 07-May-2018;9:96. Available from: http://surgicalneurologyint.com/surgicalint-articles/a-new-surgical-technique-for-the-removal-of-extensive-spinal-epidural-hydatid-cyst/
Date of Submission
20-Mar-2018
Date of Acceptance
29-Mar-2018
Date of Web Publication
07-May-2018
Abstract
Background:Extensive spinal epidural hydatidosis may contribute to extensive spinal cord compression. Multilevel laminectomy with surgical excision remains the gold standard for treating these lesions which are typically invasive, and have a high recurrence rate.
Case Description:A 35-year-old female with recurrent extensive spinal epidural hydatid cysts was treated with a limited laminectomy and uniquely with irrigation-aspiration with isotonic saline water through an epidural catheter under fluoroscopic guidance and x-ray control. The postoperative MRI documented the hydatid cysts have collapsed and the patient's paraparesis improved. She developed no disease recurrence or renewed deficits over the next 12 months.
Conclusion:Through a laminectomy, an epidural catheter may be introduced under fluoroscopic guidance/x-ray control to uniquely irrigate with isotonic saline/aspirate and decompress—the epidural hydatid cysts. This is particularly useful in patients with significant comorbidities, who are not candidates for more aggressive surgical decompression. Further, all patients should be continued on prolonged chemotherapy and should be monitored closely due to the high rate of recurrence of these cysts.
Keywords: Extradural lesion, hydatid disease, recurrence, spinal cord compression, spine, surgical treatment
INTRODUCTION
Spinal hydatid cysts are rare, and constitute less than 1% of all cases of hydatid disease. Because of their invasiveness they are highly recurrent and correlate with significant morbidity and mortality rates.[
CASE PRESENTATION
This 35-year-old female consulted developed increasing paraparesis over two preoperative months. On presentation the motor exam was 3/5, reflexes were hyperactive with bilateral Babinski responses, and she had a relative T6 pin level with loss of vibration appreciation in the lower extremities. She had been undergone surge four times in over 6 years for recurrent hydatid disease affecting the lungs and liver.
Diagnostic studies
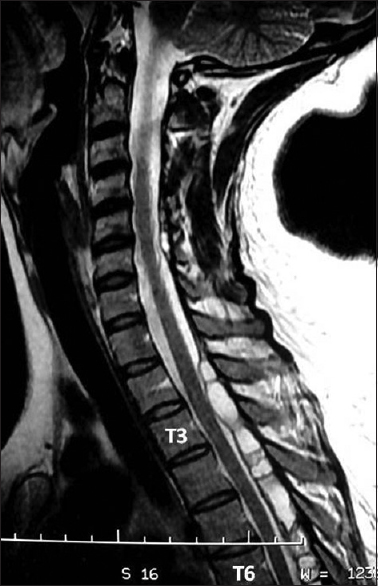
The MRI of the thoracic spine revealed several multiloculated cystic lesions (hypointense on T1-WI and brightly hyperintense on T2-WI) dorsally and epidurally in the spinal canal extending from T2 to T7 [
Surgery
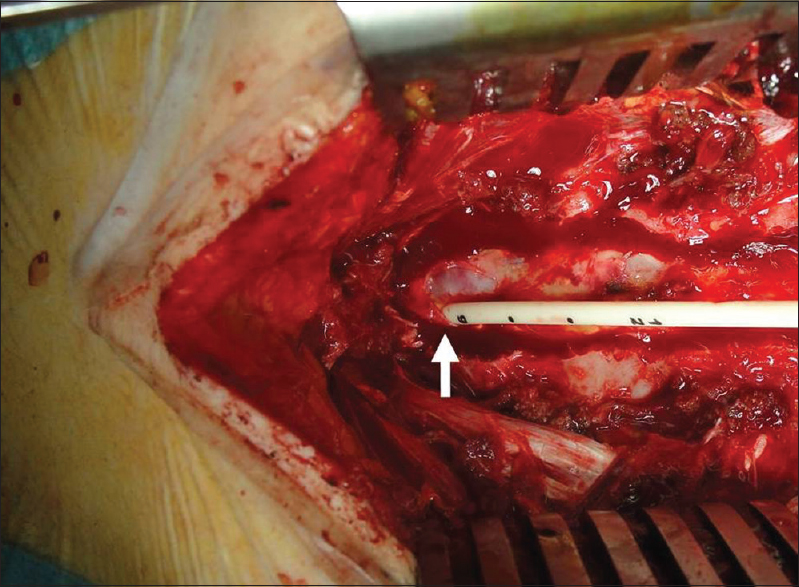
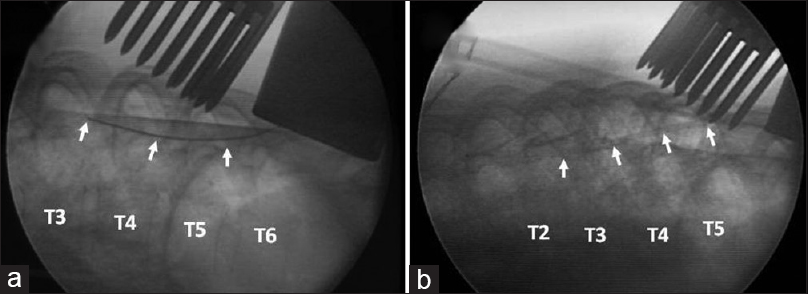
The patient underwent a T7 laminectomy. At surgery, multiple bony and extradural cysts were found and the dura was covered with thick epidural reactive tissue; the latter made the extraction of all cysts very difficult. Next, a silicon intraventricular catheter was inserted in the posterior epidural space through the T7 laminctomy, and passed/advanced cranially under fluoroscopic control to T2–T3 [Figures
Postoperative magnetic resonance
The early postoperative MRI showed near-total removal of the epidural hydatid cystic lesions [

DISCUSSION
The prognosis of spinal hydatidosis is poor, particularly if neurological deficits are present. Surgical debridement is the main stay of treatment, but this usually palliative rather than curative.[
A minimal invasive technique has been previously described in the literature to achieve spinal cord decompression via percutaneous needle aspiration. In one study, this procedure eliminated the need for emergency surgery, and provided complete resolution of the patient's quadriplegia.[
Here, the focal T7 laminectomy combined with irrigation/aspiration using a silicon catheter placed epidurally successfully resulted in decompression from T6 to T2; the MR performed the day following surgery documented collapse of all cysts.
A focal decompression (e.g., laminectomy) combined with more extensive epidural cephalad/caudad irrigation/aspiration performed under fluoroscopic guidance appears to be a viable alternative for treating extensive spinal epidural hydatid disease. Anticipated complications include; violation of the dura with subsequent spinal cord damage, CSF leak, and the development of intradural cysts; these can largely be avoided utilizing intraoperative fluoroscopic guidance.
CONCLUSION
Utilizing a focal decompression (e.g., 1–2 level laminectomy) combined with a unique irrigation-aspiration technique (e.g., shunt catheter passed cephalad caudad using isotonic saline water and aspiration) may successfully remove/decompress multilevel spinal epidural hydatid cysts. However, all patients should continue prolonged chemotherapy and be carefully monitored for recurrent disease with MR.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Akhaddar A.editorsAtlas of Infections in Neurosurgery and Spinal Surgery. Switzerland: Springer International Publishing; 2017. p. 299-310
2. Bilgic S, Kose O, Sehirlioglu A, Safaz I, Ozkan H. Primary paraspinal hydatid cyst treated with puncture, aspiration, injection and re-aspiration (PAIR) technique: A case report. Eur Spine J. 2008. 18: 165-7
3. Khazim R, Fares Y, Heras-Palou C, Ruiz Barnes P. Posterior decompression of spinal hydatidosis: Long term results. Fundacion Jimenez Diaz, Madrid, Spain. Clin Neurol Neurosurg. 2003. 105: 209-14
4. Ozdemir O, Calisaneller T, Yildirim E, Altinors N. Percutaneous CT-guided treatment of recurrent spinal cyst hydatid. Turk Neurosurg. 2011. 21: 685-7
5. Schnepper GD, Johnson WD. Recurrent spinal hydatidosis in North America. Case report and review of the literature. Neurosurg Focus. 2004. 17: 1-6
6. Spektor S, Gomori JM, Beni-Adani L, Constantini S. Spinal echinococcal cyst: Treatment using computerized tomography-guided needle aspiration and hypertonic saline irrigation. J Neurosurgery. 1997. 87: 464-7

