

- Department of Biomedicine Neurosciences and Advanced Diagnostics, School of Medicine, University of Palermo, Italy.
- Department of Scienze per la Promozione della Salute e Materno Infantile, Pathology Unit, University of Palermo, Italy.
- Department of Neurosciences and Emergency, Division of Neurosurgery, Villa Sofia Hospital, Palermo, Italy.
Correspondence Address:
Giuseppe Roberto Giammalva
Department of Biomedicine Neurosciences and Advanced Diagnostics, School of Medicine, University of Palermo, Italy.
DOI:10.25259/SNI_951_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Claudia Gaggiotti1, Giuseppe Roberto Giammalva1, Marco Raimondi2, Ada Maria Florena2, Rosa Maria Gerardi1, Francesca Graziano1, Silvana Tumbiolo3, Domenico Gerardo Iacopino1, Rosario Maugeri1. A rare diagnosis of an extraventricular neurocytoma. 08-Mar-2021;12:88
How to cite this URL: Claudia Gaggiotti1, Giuseppe Roberto Giammalva1, Marco Raimondi2, Ada Maria Florena2, Rosa Maria Gerardi1, Francesca Graziano1, Silvana Tumbiolo3, Domenico Gerardo Iacopino1, Rosario Maugeri1. A rare diagnosis of an extraventricular neurocytoma. 08-Mar-2021;12:88. Available from: https://surgicalneurologyint.com/surgicalint-articles/10635/
Date of Submission
28-Dec-2020
Date of Acceptance
09-Feb-2021
Date of Web Publication
08-Mar-2021
Abstract
Background: Extraventricular neurocytoma (EVN) is an extremely rare neoplasm of the central nervous system. As reported, it arises in a variety of locations, but mainly within the cerebral hemispheres. Despite its histological similarity with central neurocytoma (CN), EVN occurs outside the ventricular system and, in 2007, was recognized by the World Health Organization as a separate entity.
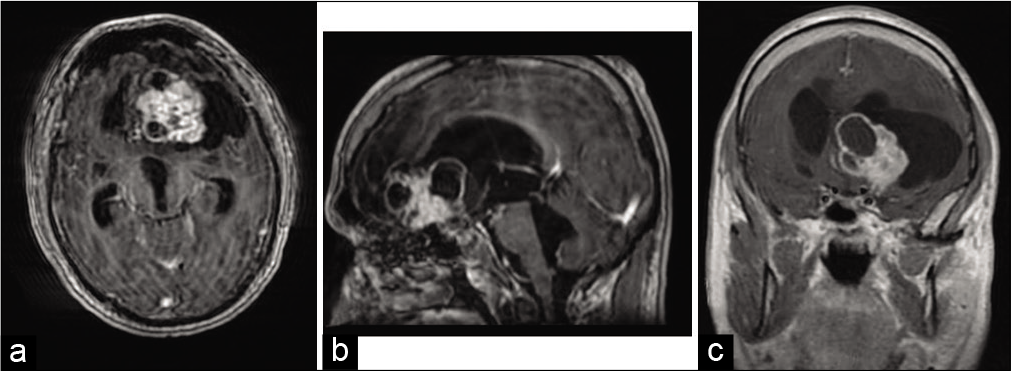
Case Description: A 39-year-old man, with a ventriculoperitoneal shunt inserted for communicating hydrocephalus, was admitted at our Unit of Neurosurgery with a 1-month history of gait disturbance, postural instability, speech disorders, and occasional incontinence. Computed tomography scan and magnetic resonance imaging showed a mixed-density neoplasm in the left frontotemporal area, with anterior cerebral falx shift, and perilesional edema. The patient underwent surgical procedure; microsurgical excision of the lesion was performed through left pterional approach. Histopathological and immunohistochemical examination revealed monomorphic round cells of the neuronal lineage, with a percentage of Ki-67 positive nuclei
Conclusion: Because of their rarity, clinical, radiologic, and histopathological characteristics of EVNs are not yet well defined, as well as the optimal therapeutic management. Whereas EVNs are rarely described in literature, we aimed to share and discuss our experience along with a review of the published literature.
Keywords: Extraventricular neurocytoma, Neurocytoma, Neuronal tumors
INTRODUCTION
Extraventricular neurocytoma (EVN) is an extremely rare neuronal tumor with just approximately 100 reported cases in literature;[
In facts, neurocytic neoplasms generally arise within the lateral ventricles and they are occasionally located in the context of brain parenchyma, without any continuity to the ventricular system. Compared with CN, EVN shows similar histopathological characteristics but a wider spectrum of locations and morphological features; both CN and EVN usually presents an indolent behavior, even though, since in 1989 Ferreol et al. described the first case of EVN, a higher rate of recurrence was observed in the latter.[
Apart from systematic reviews, published literature on EVNs consists of sporadic case reports and a few small case-series. In consideration of the low number of reports, we aim to share our experience and describe a case of a 39-year-old patient with a left frontotemporal EVN.
CASE DESCRIPTION
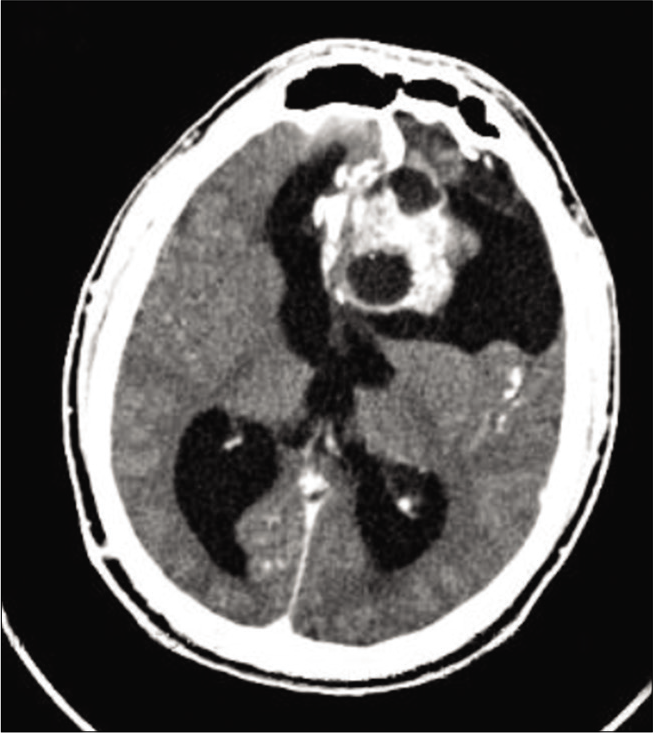
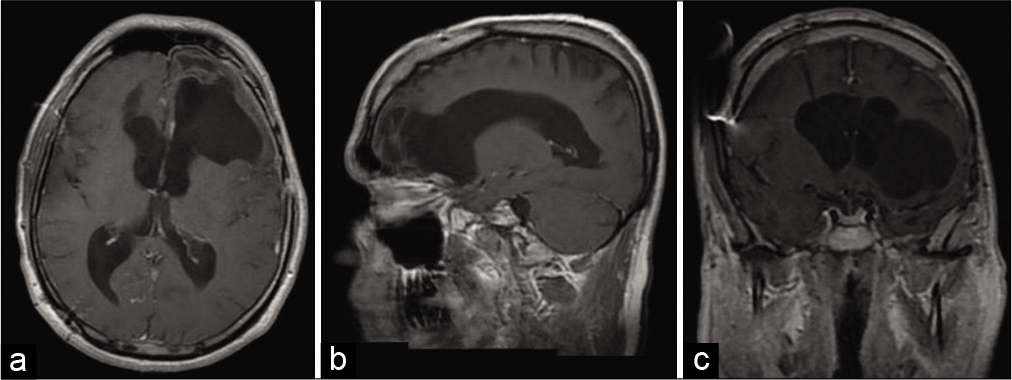
A 39-years-old man was admitted to the emergency room of our Institution for a 1-month history of gait disturbance, postural instability, speech disturbance, and episodes of incontinence. His history was remarkable for communicating hydrocephalus, which had been surgically treated at the age of 14 months with the placement of a ventriculoperitoneal shunt, followed by a distal shunt revision at the age of 16 years. At the admission, brain computed tomography (CT) scan was performed and it showed the presence of 5 cm mixed-density pseudonodular lesion. His neurological examination revealed temporospatial disorientation, absence of focal motor deficits and sensory alteration, normal and symmetrical osteotendinous reflexes, walk of little steps, and wide-based gait, several body oscillations during the Romberg’s test. A contrast-enhanced brain CT study [
Surgical procedure was performed with the aid of optic neuronavigation, intraoperative monitoring and the resection was performed though a left pterional approach.[
Fragments of the lesion were sent for pathological examination, which revealed a population of neuronal lineage (Sinaptophysin+, neuron specific enolase+, glial fibrillary acid protein−) consisting of roundish monomorphic cells mixed with a proliferation of capillary vessels and the presence of widespread calcifications; the Ki-67 index was <5%, there was no evidence of mitosis or areas of necrosis. Histopathological and immunohistochemical pattern, according to radiological findings, was consistent with a diagnosis of EVN, classified by the WHO as a Grade II tumor [
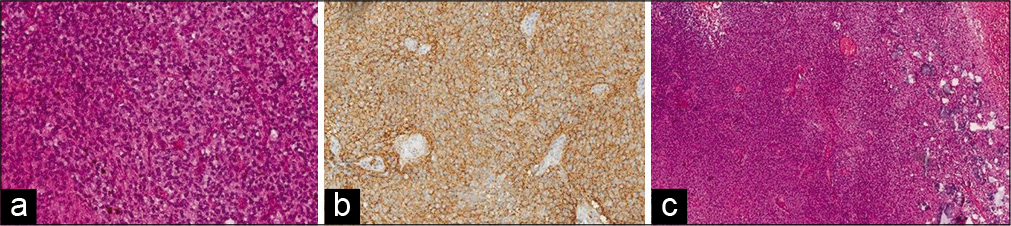
Figure 3:
(a) On low power histopathological examination, sheets of monomorphic round cells interspersed by fine capillary channels and laminated concentric microcalcification, without evidence of ischemic necrosis or hemorrhage. (hematoxylin and eosin [H and E] ×40), (b) Higher magnification shows round cells with stippled chromatin arranged in a background of finely fibrillar neuropil cores (hematoxylin and eosin [H and E] ×250), (c) strong immunoreaction for synaptophysin expressed by tumor cells (avidin-biotin ×250).
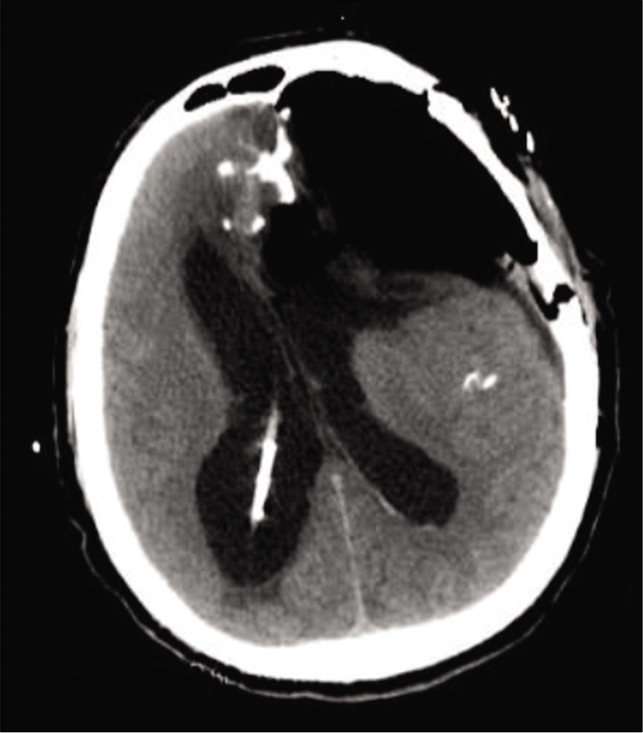
The postoperative course was uneventful and control CT scan [
After the hospital discharge patient underwent at home neurorehabilitation with consistent improvement of his gait and speech. He also underwent adjuvant radiotherapy and at the present his follow-up is still ongoing.
DISCUSSION
Although the exact incidence is still not precisely defined, in a systematic review the incidence of cerebral EVN has been estimated to be 0.13% of approximately 7000 cases of intracranial tumors.[
EVNs may occur in various site outside the ventricular system; the most common location reported is the frontal lobe, followed by the parietal, temporal, and occipital lobes.[
Clinical presentation of EVN is heterogeneous, non-specific and it varies depending on the location of the tumor and the mass effect exerted.[
In our case, the radiologic features of patient’s lesion are consistent with the previous reports.[
However, EVNs may exhibit a wealth of non-specific imaging features, leading to a difficult differential diagnosis mainly toward oligodendrogliomas and oligoastrocytomas with neurocytic differentiation, ganglioglioma, pilocytic astrocytoma, ependymoma, and dysembryoblastic neuroepithelial tumors.[
Furthermore, CNs and EVNs exhibit a shared microscopic appearance. In facts, neurocytic neoplasms are mainly composed of uniform roundish cells with neuronal differentiation, strongly immunoreactive for synaptophysin. EVN, however, has been described with a wider spectrum of proliferation rates and cellularity, showing tendency for ganglionic or glial differentiation; in 2001, Brat et al. proposed “atypical EVN,” a variant associated with a higher recurrence rate.[
In our patient, histopathological examination revealed low Ki-67 index without evidence of mitotic activity or necrosis, while proliferation of capillary vessels was observed. Age and atypical histological features have been suggested as negative prognostic factors associated with poorer outcomes.[
The therapeutic management for EVNs is based on surgical removal, while radiotherapy or chemotherapy should be considered in cases of subtotal resection or as salvage for local recurrence after surgery. Compared with gross total resection, subtotal resection followed by radiotherapy may offer a reasonably good outcome with a similar overall survival.[
Nevertheless, Dutta et al. recently investigated different patterns of care in a large cohort of patients with diagnosed neurocytomas, founding that tumor location and use of radiation were not predictive for improved survival.[
CONCLUSION
Since they are rare tumors, clinical, radiologic, and histopathological characteristics of EVNs are not yet well defined, as well as the optimal therapeutic management. Whereas EVNs are rarely described in the literature, we described our singular case of extra-ventricular neurocytoma, with our surgical management and an exhaustive review of the published literature.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Barone F, Alberio N, Iacopino D, Giammalva G, D’Arrigo C, Tagnese W. Brain mapping as helpful tool in brain glioma surgical treatment-toward the “perfect surgery”?. Brain Sci. 2018. 8: 192
2. Brat DJ, Scheithauer BW, Eberhart CG, Burger PC. Extraventricular neurocytomas: Pathologic features and clinical outcome. Am J Surg Pathol. 2001. 25: 1252-60
3. Chen F, Jin R, Wu X, Dong Z, Chen D. Extraventricular neurocytoma in the left frontal lobe: A case report and literature review. World Neurosurg. 2018. 112: 178-81
4. Dutta SW, Kaleem TA, Muller DA, Peterson J, Harrell AC, Quinones-Hinojosa A. Central neurocytoma: Clinical characteristics, patterns of care, and survival. J Clin Neurosci. 2018. 53: 106-11
5. Enam SA, Rosenblum ML, Ho KL. Neurocytoma in the cerebellum. Case report. J Neurosurg. 1997. 87: 100-2
6. Ersoz S, Kucuk H, Mungan S, Turgutalp H, Imamoglu M, Kosucu P. Neurocytoma arising in an adrenal gland mature teratoma. Fetal Pediatr Pathol. 2011. 30: 275-9
7. Ferreol E, Sawayal R, de Courten-Myers GM. Primary cerebral neuroblastoma (neurocytoma) in adults. J Neurooncol. 1989. 7: 121-8
8. Francaviglia N, Iacopino DG, Costantino G, Villa A, Impallaria P, Meli F. Fluorescein for resection of high-grade gliomas: A safety study control in a single center and review of the literature. Surg Neurol Int. 2017. 8: 145
9. Friedrichs N, Vorreuther R, Fischer HP, Wiestler OD, Buettner R. Neurocytoma arising in the pelvis. Virchows Arch. 2003. 443: 217-9
10. Giammalva GR, Iacopino DG, Azzarello G, Gaggiotti C, Graziano F, Gulì C. End-of-life care in high-grade glioma patients. The palliative and supportive perspective. Brain Sci. 2018. 8: 125
11. Hirschowitz L, Ansari A, Cahill DJ, Bamford DS, Love S. Central neurocytoma arising within a mature cystic teratoma of the ovary. Int J Gynecol Pathol. 1997. 16: 176-9
12. Hu JR, Li J, Lv GH, Deng YW, Zou MX. Extraventricular neurocytoma mimicking bone tumor in thoracic spinal column. Spine J. 2015. 15: e65-6
13. Jiang M, Long L, Zeng J, Meng W, Zee CS. Imaging characteristics of cerebral extraventricular neurocytoma with pathological correlation. J Neurooncol. 2018. 140: 289-96
14. Kane AJ, Sughrue ME, Rutkowski MJ, Aranda D, Mills SA, Lehil M. Atypia predicting prognosis for intracranial extraventricular neurocytomas. J Neurosurg. 2012. 116: 349-54
15. Kapoor N, Gandhi A, Chaurasia AK. Central neurocytoma in the vermis of the cerebellum. Indian J Pathol Microbiol. 2009. 52: 108-9
16. Kawaji H, Saito O, Amano S, Kasahara M, Baba S, Namba H. Extraventricular neurocytoma of the sellar region with spinal dissemination. Brain Tumor Pathol. 2014. 31: 51-6
17. la Torre D, Maugeri R, Angileri FF, Pezzino G, Conti A, Cardali SM. Human leukocyte antigen frequency in human high-grade gliomas: A case-control study in Sicily. Neurosurgery. 2009. 64: 1082-8
18. Liu K, Wen G, Lv XF, Deng YJ, Deng YJ, Hou GQ. MR imaging of cerebral extraventricular neurocytoma: A report of 9 cases. Am J Neuroradiol. 2013. 34: 541-6
19. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007. 114: 97-109
20. Louis DN, Perry A, Reifenberger G, von Deimling A, FigarellaBranger D, Cavenee WK. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016. 131: 803-20
21. Mallick S, Benson R, Rath G. Patterns of care and survival outcomes in patients with an extraventricular neurocytoma: An individual patient data analysis of 201 cases. Neurol India. 2018. 66: 362-7
22. Maugeri R, Villa A, Pino M, Imperato A, Giammalva GR, Costantino G. With a little help from my friends: The role of intraoperative fluorescent dyes in the surgical management of high-grade gliomas. Brain Sci. 2018. 8: 31
23. Patil AS, Menon G, Easwer HV, Nair S. Extraventricular neurocytoma, a comprehensive review. Acta Neurochir (Wien). 2014. 156: 349-54
24. Pino MA, Imperato A, Musca I, Maugeri R, Giammalva GR, Costantino G. New hope in brain glioma surgery: The role of intraoperative ultrasound. A review. Brain Sci. 2018. 8: 202
25. Raja AI, Yeaney GA, Jakacki RI, Hamilton RL, Pollack IF. Extraventricular neurocytoma in neurofibromatosis Type 1: Case report. J Neurosurg Pediatr. 2008. 2: 63-7
26. Romano N, Federici M, Castaldi A. Imaging of extraventricular neurocytoma: A systematic literature review. Radiol Med. 2020. 125: 961-70
27. Rusiecki D, Lach B, Manoranjan B, Fleming A, Ajani O, Singh SK. Progression of atypical extraventricular neurocytoma to anaplastic ganglioglioma. Hum Pathol. 2017. 59: 125-30
28. Sakurada K, Akasaka M, Kuchiki H, Saino M, Mori W, Sato S. A rare case of extraventricular neurocytoma. Brain Tumor Pathol. 2007. 24: 19-23
29. Sharma MC, Deb P, Sharma S, Sarkar C. Neurocytoma: A comprehensive review. Neurosurg Rev. 2006. 29: 270-85
30. Singh A, Chand K, Singh H, Sarkar C, Sharma MC. Atypical neurocytoma of the spinal cord in a young child. Childs Nerv Syst. 2007. 23: 207-11
31. Tsai CY, Tsai TH, Lin CH, Cheng YH, Lieu AS. Unusual exophytic neurocytoma of thoracic spine mimicking meningioma: A case report and review of the literature. Eur Spine J. 2011. 20: S239-42
32. Umana GE, Alberio N, Amico P, Lavecchia A, Fagone S, Fricia M.editors. Giant Cystic Brain Metastasis from Ovarian Papillary Serous Adenocarcinoma: Case Report and Review of the Literature, Interdisciplinary Neurosurgery: Advanced Techniques and Case Management. 2020. p.
33. Umana GE, Raudino G, Alberio N, Inserra F, Giovinazzo G, Fricia M. Slit-like hypertensive hydrocephalus: Report of a late, complex, and multifactorial complication in an oncologic patient. Surg Neurol Int. 2020. 11: 219
34. von Koch CS, Schmidt MH, Uyehara-Lock JH, Berger MS, Chang SM. The role of PCV chemotherapy in the treatment of central neurocytoma: Illustration of a case and review of the literature. Surg Neurol. 2003. 60: 560-5
35. Wang YY, Kearney T, du Plessis D, Gnanalingham KK. Extraventricular neurocytoma of the sellar region. Br J Neurosurg. 2012. 26: 420-2
36. Xiong Z, Zhang J, Li Z, Jiang J, Han Q, Sun S. A comparative study of intraventricular central neurocytomas and extraventricular neurocytomas. J Neurooncol. 2015. 121: 521-9
37. Yi KS, Sohn CH, Yun TJ, Choi SH, Kim JH, Han MH. MR imaging findings of extraventricular neurocytoma: A series of ten patients confirmed by immunohistochemistry of IDH1 gene mutation. Acta Neurochir (Wien). 2012. 154: 1973-9

